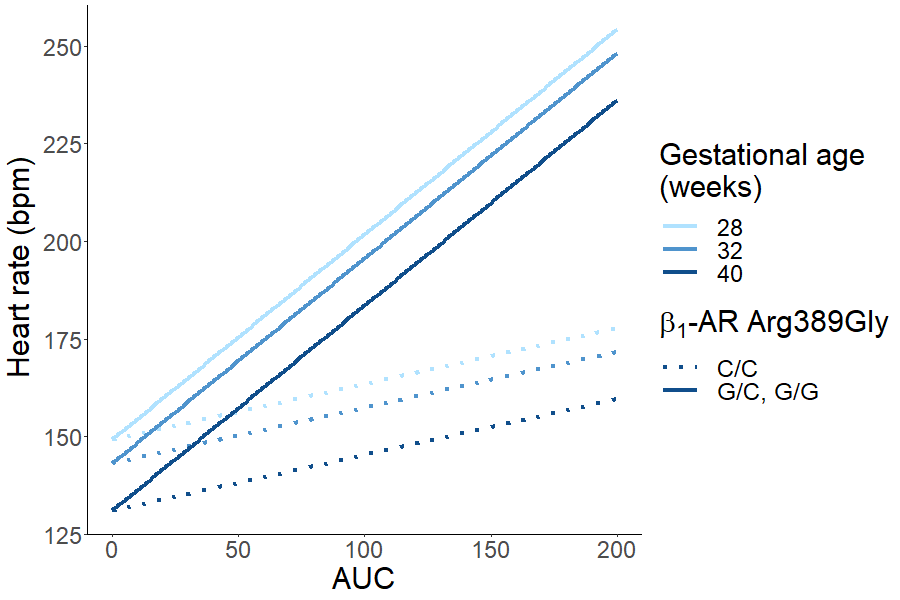
Aim: To determine whether the known single nucleotide polymorphisms in adrenoreceptor associated genes affect the hemodynamic response to dobutamine in critically ill neonates. Methods: Alleles in the known genetic single nucleotide polymorphisms in β1 and β2 adrenoceptor (AR) genes and Gs protein α-subunit gene (GNAS) possibly affecting inotropic effect were identified in patients of neonatal dobutamine pharmacokinetic-pharmacodynamic study. Linear mixed-effect models were used to describe the effect of genetic polymorphisms to heart rate (HR), left ventricular output (LVO) and right ventricular output (RVO) during dobutamine treatment. Results: 26 neonates (5 term, 21 preterm) were studied. Dobutamine plasma concentration and exposure time respective HR (adjusted to gestational age) is dependent on β1-AR Arg389Gly polymorphism so that in G/G (Gly) homozygotes and G/C heterozygotes dobutamine increases HR more than in C/C (Arg) homozygotes, with parameter estimate (95% CI) of 38.3 (15.8 – 60.7) bpm per AUC of 100 mg·h, p=0.0005. LVO (adjusted to antenatal glucocorticoid administration and illness severity) and RVO (adjusted to gestational age and illness severity) is dependent on GNAS c.393C>T polymorphism so that in T/T homozygotes and C/T heterozygotes but not in C/C homozygotes LVO and RVO increase with dobutamine treatment, 24.5 (6.2 – 42.9) mL kg-1 min-1 per AUC of 100 mg·h, p=0.0116 and 33.2 (12.1 – 54.3) mL kg-1 min-1 per AUC of 100 mg·h, p=0.0025, respectively. Conclusion: In critically ill neonates, β1-AR Arg389Gly and GNAS c.393C>T polymorphisms may play a role in the haemodynamic response to dobutamine during the first hours and days of life.