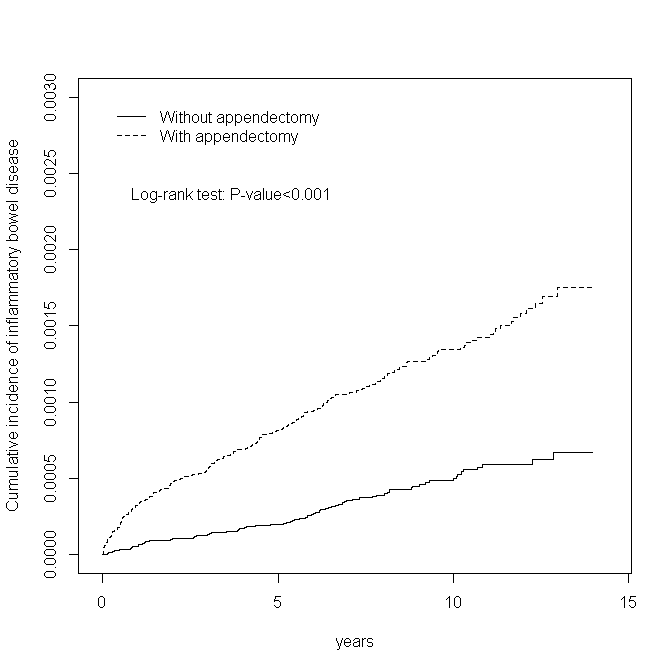
Aim: The appendix has a complicated immune function, and appendectomy may derange the immune system. Studies on the relationship between appendectomy and subsequent inflammatory bowel disease (IBD) have been inconsistent. We conducted a nationwide cohort study consisting of individuals who underwent appendectomy to evaluate the incidence and risk of ulcerative colitis (UC) and Crohn’s disease (CD). Methods: We identified patients aged >20 years who underwent appendectomy between 2000 and 2012 from inpatient claims of the National Health Insurance Research Database (NHIRD) and assigned them to the appendectomy cohort. Then, we randomly selected patients without appendectomy in the NHIRD and assigned them to the comparison cohort in a frequency-matched 1:1 ratio based on sex, age, and index year. We tracked down all participants until IBD diagnosis, death, or the end of 2013. Cox models were used to estimate the hazard ratio (HR), and 95% confidence intervals (CIs) were used to compare the IBD risk between the appendectomy and comparison cohorts. Results: The appendectomy and comparison cohorts in the study consisted of 246 562 patients each. The appendectomy cohort exhibited a 2.23- and 3.48-fold higher risk of UC (adjusted HR = 2.23, 95% CI = 1.59-3.12) and CD (adjusted HR = 3.48, 95% CI = 2.42-4.99), respectively, than did the comparison cohort. UC and CD risks significantly increased in the appendectomy cohort regardless of whether appendicitis was present. Conclusion: Our study suggests that appendectomy increases UC and CD risks irrespective of appendicitis.