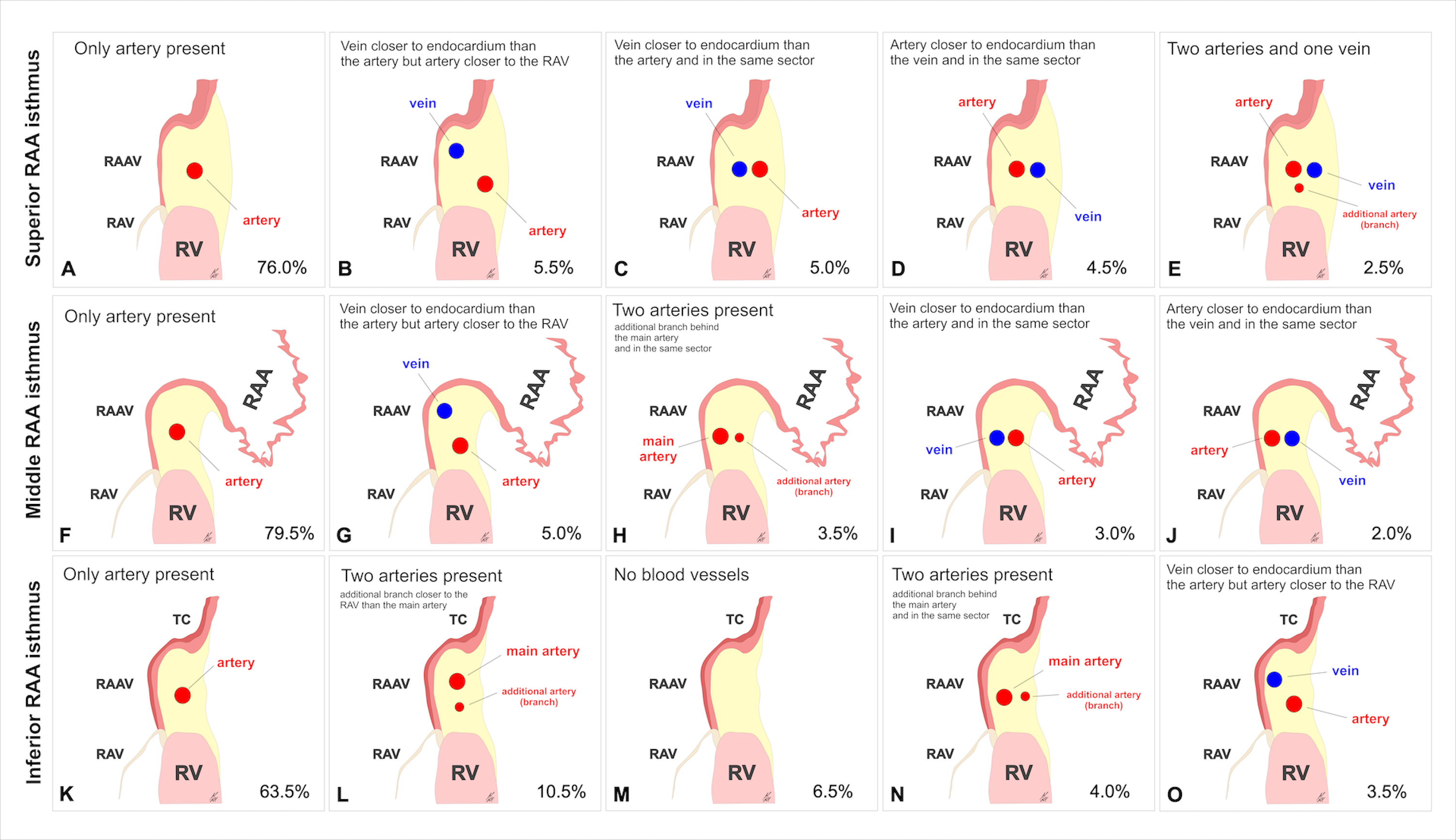
Introduction: The aim of our study was to investigate the presence and mutual relationships of coronary vessels within the right atrial appendage RAA vestibule. Methods and Results: We examined 200 autopsied hearts. The RAA vestibule was cross sectioned along its isthmuses (superior, middle, and inferior). We assessed the presence and mutual relationships between coronary blood vessels. The right coronary artery (RCA) was present in 100% of the superior RAA isthmuses but absent in 2.0% of hearts within the middle isthmus and in 6.5% of hearts within the inferior RAA isthmus. Its diameter was quite uniform along the superior (2.6±0.8mm), middle (2.9±1.1mm) and inferior (2.7±0.9mm) isthmuses (p=0.12). The location of the RCA varied significantly, and it was sometimes accompanied by other accessory coronary vessels. In all the isthmuses, the RCA ran significantly closer to the endocardial surface than to the epicardial surface (p<0.001). At the superior RAA isthmus, the artery was furthest from the right atrial endocardial surface and this distance gradually decreased between the middle RAA isthmus and the inferior RAA isthmus (9.0±4.0 vs. 6.2±3.0 vs. 4.8±2.3mm, respectively; p<0.001). The interposed RCA was found in 7.0% of cases within the superior isthmus, in 2.5% within the middle isthmus and in 1.5% within the inferior isthmus. Conclusions: This study was the most complex analysis of the mutual arrangements and morphometric characteristics of coronary blood vessels within the RAA vestibule. Awareness of additional blood vessels within the vestibule can help clinicians plan and perform safe and efficacious procedures in this region.