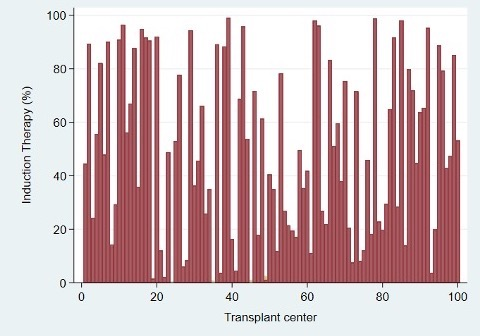
Background: Institutional factors have been shown to impact outcomes following orthotopic heart transplantation (OHT). This study evaluated center variability in the utilization of induction therapy for OHT and its implications on clinical outcomes. Methods: Adult OHT patients between 2010 and 2018 were identified from the UNOS registry. Transplant centers were stratified based on their rates of induction therapy utilization. Mixed-effects logistic regression models were created with drug-treated rejection within 1-year as primary endpoint and individual centers as random parameter. Risk-adjusted Cox regression was used to evaluate patient-level mortality outcomes. Results: In 17,524 OHTs performed at 100 centers, induction therapy was utilized in 48.6% (n=8411) with substantial variability between centers (IQR 21.4 – 79.1%).There were 36, 30, and 34 centers in the low (<29%), intermediate (29-66%), and high (>67%) induction utilization terciles groups, respectively. Induction therapy did not account for the observed variability in the treated rejection rate at 1-year among centers after adjusting for donor and recipient factors (p=0.20). No differences were observed in postoperative outcomes among induction utilization centers groups (all, p>0.05). Furthermore, there was a weak correlation between the percentage of induction therapy utilization at the center-level and recipients found to have moderate (r=0.03) or high (r=0.04) baseline risks for acute rejection at 1-year. Conclusions: This analysis demonstrates there is substantial variability in the use of induction therapy among OHT centers. In addition, there was a minimal correlation with baseline recipient risk or 1-year rejection rates, suggesting a need for better-standardized practices for induction therapy use in OHT.