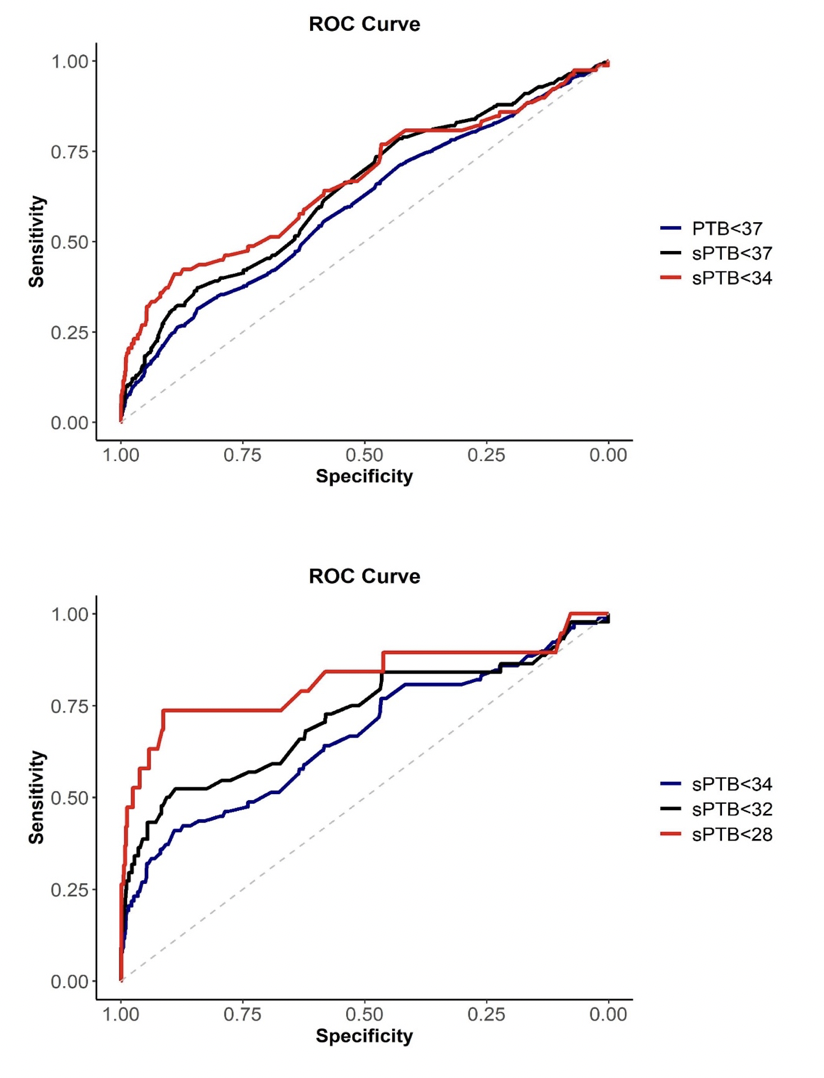
Objective: To identify the association between cervical length (CL) and gestational age at birth. Design: Prospective cohort study. Setting: Seventeen Brazilian reference hospitals. Population: A cohort of 3139 asymptomatic singleton pregnant women who participated in the screening phase of a Brazilian multicenter randomized controlled trial (P5 trial). Methods: Transvaginal ultrasound (TVU) to measure CL was performed from 18 to 22+6 weeks. Women with CL ≤ 30 mm received vaginal progesterone (200 mg/day) until 36 weeks’ gestation. Main Outcome Measures: Area under receive operating characteristic curve (AUC), sensitivity, specificity, Kaplan-Meier curves for preterm birth (PTB), number needed to screen (NNS). Results: CL ≤25mm was associated with extremely severe, severe, moderate and late PTB, whereas a CL 25–30mm was directly associated with late sPTB. The AUC to predict sPTB<28 weeks was 0.82 and for sPTB<34 weeks was 0.67. Almost half of the sPTB occurred in nulliparous women and CL ≤30mm was associated with sPTB <37 weeks (OR = 7.84; 95%CI = 5.5–11.1). The NNS to detect one sPTB <34 weeks in women with CL ≤25mm is 121 and 248 screening tests are necessary to prevent one sPTB <34 weeks using vaginal progesterone prophylaxis. Conclusions: CL measured by TVU is associated with sPTB <34 weeks. Women with CL ≤30mm are at increased risk for late sPTB. Funding: Bill & Melinda Gates Foundation [OPP1107597], the Brazilian Ministry of Health, and the Brazilian National Council for Scientific and Technological Development (CNPq) [401615/20138]. Keywords: cervical length; number needed to screen; preterm birth; short cervix.