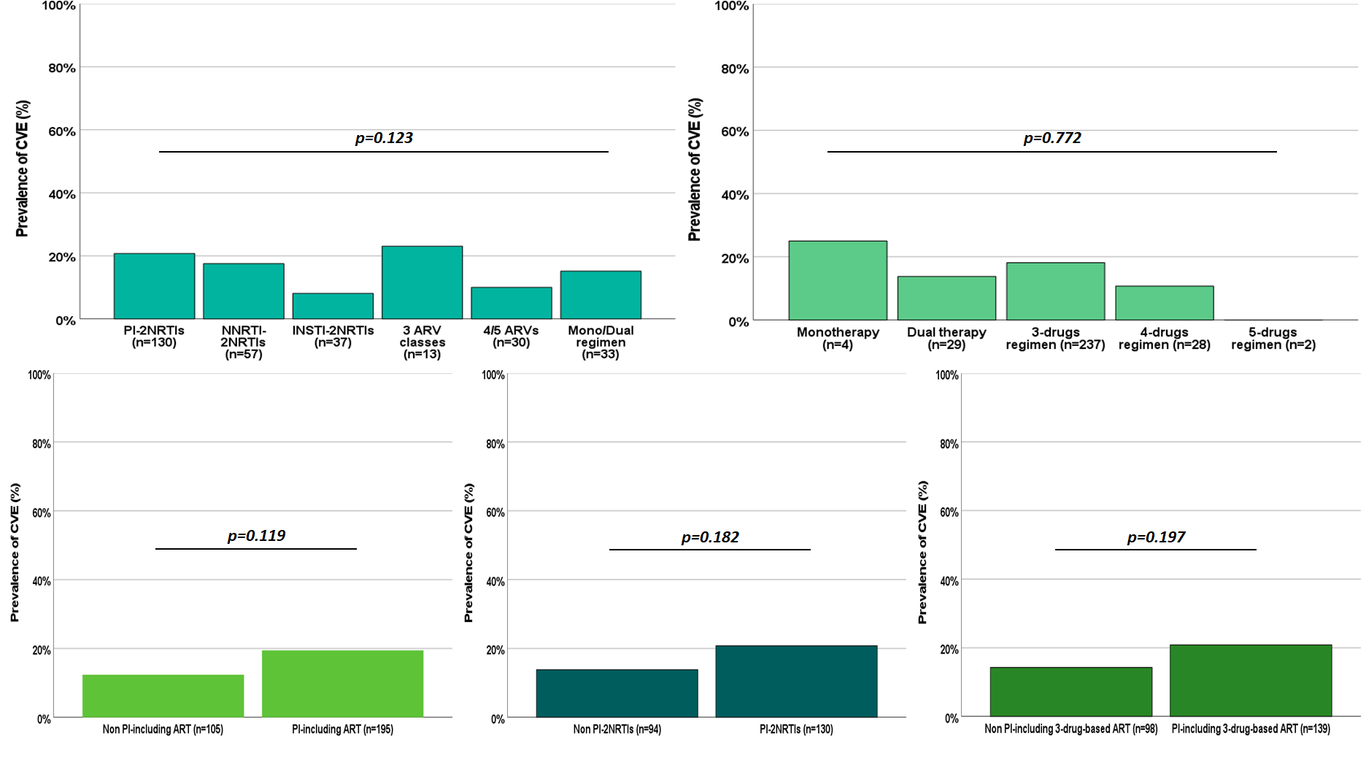
Background: We assessed whether the association between the risk of cerebrospinal fluid escape (CVE) and specific antiretroviral (ARV) classes, such as protease inhibitors, is due to suboptimal pharmacological profile generated by archived resistance-associated mutations (RAMs). Methods: A retrospective multicentric study on 300 adult people with HIV on antiretroviral therapy (ART) and available historical plasma genotype resistance testing (HGRT) for reverse transcriptase (RT) and protease genes between 2001 and 2021. The odds ratio for demographic, clinic-, and ART-related variables and CVE was estimated by multivariable modelling. HGRT-adjusted central nervous system effectiveness penetration (CPE) score was computed in modelling the risk. Results: Median age, plasma VL, and CD4 count were 49 years, <50 copies/mL, and 310 cells/μL. CVE was detected in 51 participants (17.0%). No difference in CVE prevalence was observed according to ART type, number of ARVs or ARV classes. Participants with CVE had more frequently plasma (52.9% vs 32.1%, p=0.005) and CSF RAMs in RT (n=63, 57.1% vs 28.6%, p=0.029), but not in protease gene. The presence of plasma RAMs in RT associated with increased odds of CVE in adjusted analyses (aOR 3.9, p<0.001) and in models restricted to plasma viral load ≤50 copies/mL (n=202; aOR 4.3 , p=0.003). CVE risk decreased by 40% per each point increase in HGRT-adjusted CPE score in multivariable models (p<0.001). Conclusions: Viruses harboring mutations appear to favor CVE and the impact of single ARV classes or type of ART regimens may lose significance when adjusted for the presence and effect of specific RAMs.