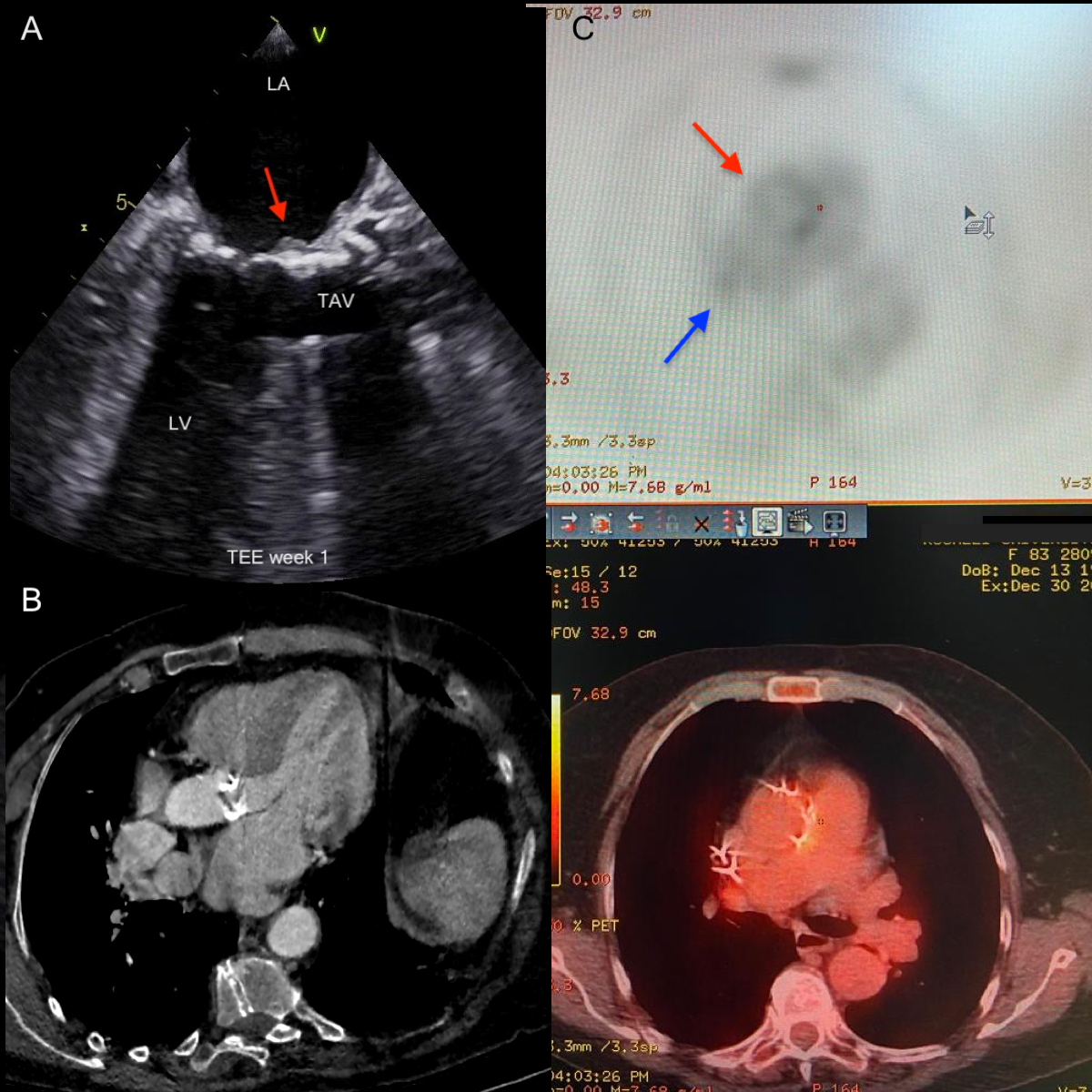
Abstract With the increasing number of transcatheter aortic valve implantations (TAVI) being performed comes a need to better understand TAVI-associated complications such as infective endocarditis (IE), leaflet thrombosis, and paravalvular regurgitation. An 83 year-old women, who had undergone TAVI followed by permanent pacemaker implantation 3 months before, presented to outpatient clinic with fever lasting for 5 days. History revealed that fever reached 39°C and was subsided by the initiation of amoxycillin/clavulinic acid prescribed by her family physician. Transesophageal echocardiography (TEE) revealed normal aortic leaflet thickness and motion. A mass at aorto-mitral continuity in left atrium was detected (Figure 1A, Video 1). The mass was heterogenous, 8×3 mm in size, and did not have visual characteristics of vegetation. Mitral valve seemed unaffected. There was no mitral regurgitation. No paravalvular abscess, pseudoaneurysm, or fistula was detected. We had confirmed that the mass was not present before the TAVI after reviewing preprocedural computed tomography (CT) scan (Figure 1B). There was fluorodeoxyglucose uptake around TAV and permanent pacemaker leads in positron emission computed tomography (Figure 1C). With the fever early after TAVI and a suspicious mass adjacent to TAV, we decided to treat the patient as “possible IE” according to modified Duke criteria. A 6-week therapy of vancomycine plus rifampin accompanied by 2-week therapy of gentamycine was initiated. The first set of blood cultures turned out to be negative. Second set of blood cultures were also negative at the second week of hospitalization. TEE was repeated at the 3rd and 5th weeks and showed identical findings to the first TEE (Figure 2, Video 2-3). Clinical condition of the patient was very good. She did not develop fever after hospitalization. The patient was discharged uneventfully after 6 weeks of antibiotic therapy. We had concluded that the mass could be thrombus in origin. After 6 motnhs of warfarin plus clopidogrel therapy control TEE revealed that the mass at aorto-mitral continuity had disappeared, mitral valve was normal, TAV was normal with similar valvular gradient and had trivial paravalvular regurgitation identical to initial examinations (Figure 2, Video 4). There was no finding of paravalvular abscess, pseudoaneurysm, or fistula. The patient was still asymptomatic with good functional capacity and TTE showed normal valvular function at 1-year followup of TAVI.