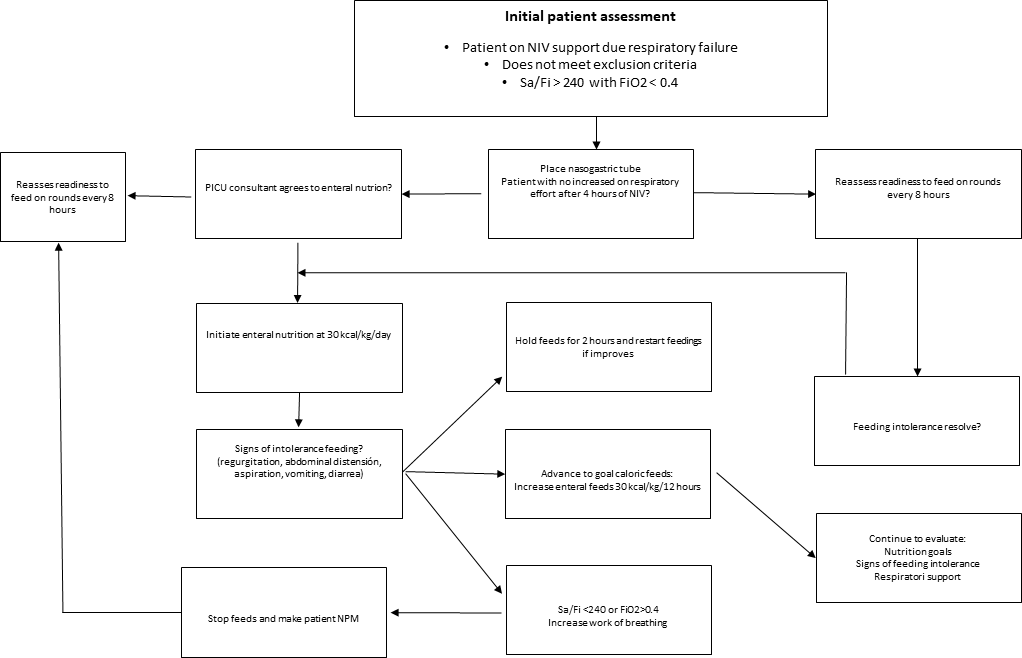
Purpose: Children with bronchiolitis admiteed to the pediatric intensive care unit (PICU) for acute respiratory failure may require respiratory support with non-invasive ventilation (NIV). Enteral nutrition (EN) is associated with a reduction in hospital stay. Even so, guidelines do not specify on how to initiate, increase and maintain EN in these patients. Methods This was a prospective interventional study. Inclusion criteria were patients with bronchiolitis under NIV. A multidisciplinary team created an algorithm to improve EN for critically ill patients with bronchiolitis in need of NIV. In order to assess the protocol implementation, two periods of time were compared: Group 1: without nutrition implementation protocol vs Group 2, once the protocol was implemented. The project aim was to decrease the mean time to EN initation by 50% after the start of NIV. Secondary endpoints were time to reach target calories ( 100 kcal/kg/day), NIV duration, and % of patients with adverse effects. Results Hundred two patients were included in this study. In group 1, Forty eight and 54 in group 2. Statistically significant differences were detected in the main outcome. The mean time until the start of EN decreased from 18.5 hours to 6 hours (p<0.05) Median time to reach calorie goal decreased from 103.5 hours to 48.5 hours (p<0.05). No differences were dettected in other outcomes. Conclusions The implementation of a standardized route for EN in patients with NIV allow a decrease in the time of the start feeds and the time to the goal of caloric enteral nutrition.