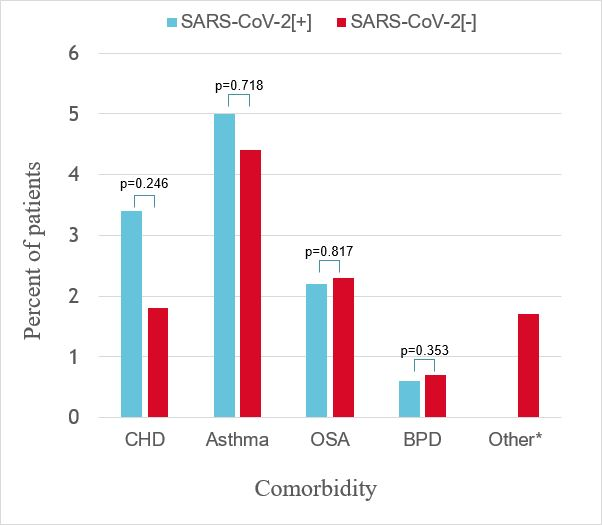
Background There are limited data in paediatric populations evaluating whether chronic cardiorespiratory conditions are associated with increased risk of COVID-19. We aimed to compare the rates of chronic cardiac and respiratory disease in children testing positive (SARS-CoV-2[+]) compared to those testing negative (SARS-CoV-2[-]) at our institution. Method Prospective cohort with nested case-control study of all children tested by PCR for SARS-CoV-2 by nasopharyngeal/oropharyngeal sampling between March and October 2020. Children were identified prospectively via laboratory notification with age and sex-matching of SARS-CoV-2[+] to SARS-CoV-2[-] (1:2). Clinical data were extracted from the electronic medical record. Results In total, 179 SARS-CoV-2[+] children (44% female, median age 3.5 yrs, range 0.1 to 19.0 yrs) were matched to 391 SARS-CoV-2[-] children (42% female, median age 3.7 yrs, range 0.1 to 18.3 yrs). The commonest co-morbidities showed similar frequencies in the SARS-CoV-2[+] and [-] groups: asthma (n = 9, 5% vs n = 17, 4.4%, p = 0.71), congenital heart disease (n = 6, 3.4% vs n = 7, 1.8%, p = 0.25) and obstructive sleep apnoea (n = 4, 2.2% vs n = 10, 2.3%, p = 0.82). In the SARS-CoV-2 group, the prevalence of symptomatic disease was similar amongst children with and without cardiorespiratory comorbidities (n = 12, 75% vs n = 103, 57%, p = 0.35) who tested positive. A high proportion of children hospitalised with SARS-CoV-2 infection had cardiac comorbidities (23.8%). Conclusions In this single site dataset, rates of pre-existing cardiorespiratory disease were similar in SARS-CoV-2[+] and SARS-CoV-2[-] children. High rates of comorbid cardiac disease were observed amongst hospitalised children with COVID-19, warranting further research to inform public health measures and vaccine prioritisation.