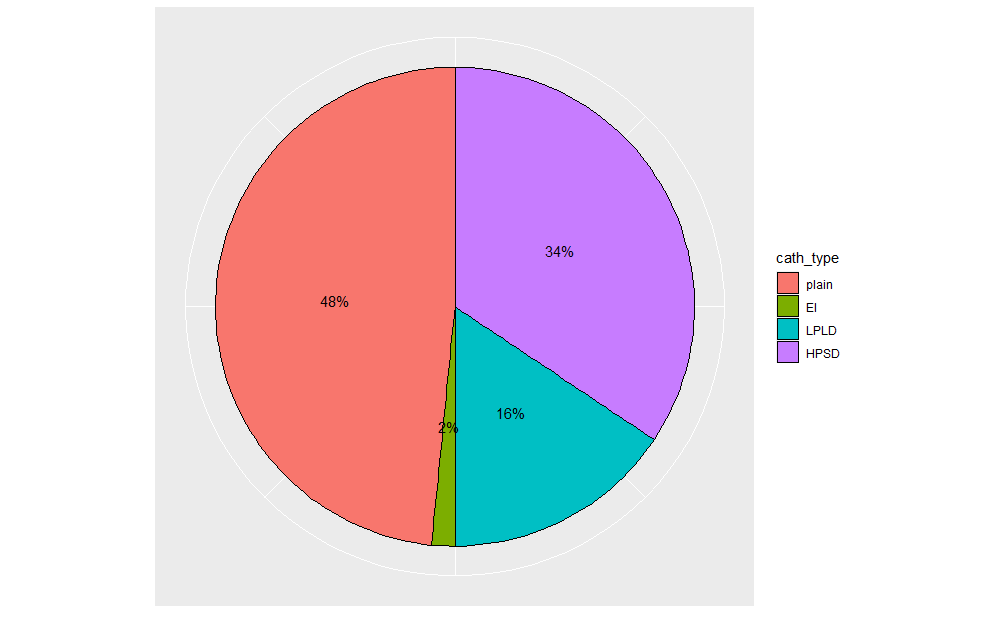
Introduction Atrioventricular node (AVN) radiofrequency ablation is a highly effective treatment of atrial tachycardias resistant to other management modalities. There are limited studies that compare different radiofrequency ablation catheters. Our study aimed to compare the effectiveness of several types of ablation catheters in AVN ablation. Methods We identified patients who underwent AVN ablation for different indications at our institution. Data related to patients and procedures were collected through retrospective chart review. The radiofrequency catheters used were: plain non irrigated, externally irrigated (EI), and contact force sensing with 10-20 gm of force in two different settings: low power long duration (LPLD) (30W, 45°C, and 60 sec) and high-power short duration (HPSD) (50W, 43°C, and 12 sec). We compared the different catheters in terms of success rate using logistic regression and lesion time using linear regression. Results We identified 66 patients who underwent AVN ablation, out of which 31 were female (47%). The patients were elderly, with a mean age of 73.27 years. The indications were resistant atrial fibrillation in 74%, atrial flutter in 18%, and other atrial tachycardias in 8% of patients. Types of catheters used were plain non irrigated in 48%, EI in 2%, LPLD in 16%, and HPSD in 34% of patients. All ablation procedures were successful with no immediate post-procedure complications. Regarding lesion time, HPSD was significantly shorter compared to plain catheters by 403.42s[-631.67, -175.17]. Conclusions Radiofrequency ablation of AVN is a highly effective treatment modality for atrial tachyarrhythmias that failed other management methods. While plain catheter, LPLD, and HPSD were equally safe and effective, HPSD catheter had significantly shorter lesion time and thus procedure time.