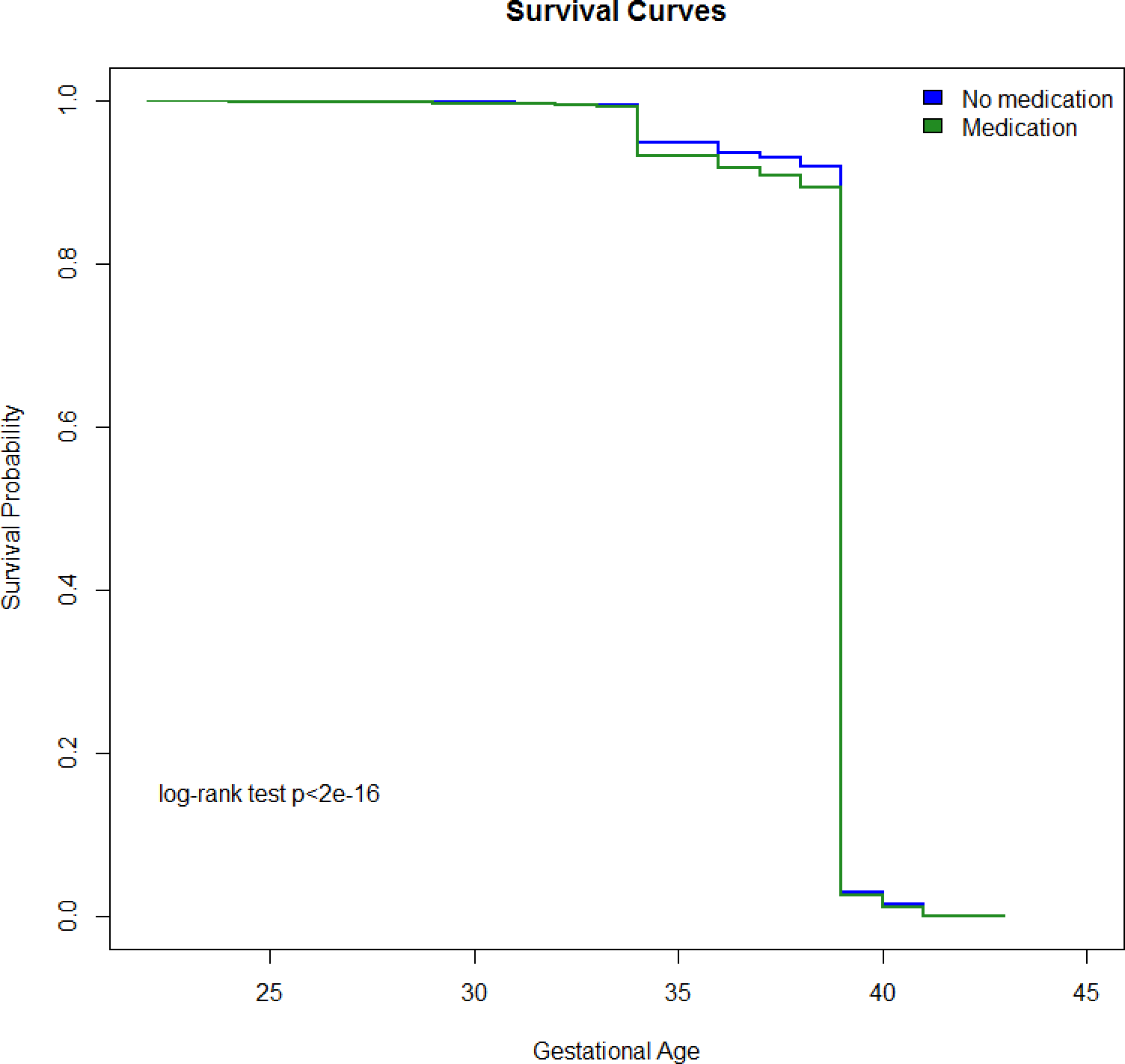
Objective: To determine the association between treatment of persistent BV in pregnancy and risk for spontaneous preterm birth (sPTB). Design: The retrospective data from IBM® MarketScan® Commercial Database was analyzed. Setting: United States outpatient data. Population or Sample: Women aged 12–55 years with a singleton gestation. Methods: Women were linked to an outpatient medications database and medications taken during the pregnancy were analyzed. Treatment of BV in pregnancy was defined as a diagnosis of BV and treatment with Metronidazole and/or Clindamycin, and persistent treatment of BV was defined as BV in more than 1 trimester or BV requiring more than 1 antibiotic prescription. Odds ratios were calculated comparing sPTB in those with BV and persistent BV to women without BV in pregnancy. Survival analysis using Kaplan-Meier curves for the gestational age at delivery was also performed. Main outcome measures: sPTB Results: Among a cohort of 2,538,606 women, 216,611 had an associated ICD-9 or ICD-10 code for diagnosis of BV alone, and 63,817 had BV and were treated with either metronidazole and/or clindamycin. The sPTB rate among women treated with BV was 7.5% compared with 5.7% for women without BV who did not receive antibiotics. Relative to those without BV in pregnancy, odds ratios for sPTB were highest in those treated for BV in both the first and second trimester (1.66 [95% CI 1.52, 1.81]) or those with 3 or more prescriptions in pregnancy (1.48 [95% CI 1.35, 1.63]. Conclusions: Treatment of persistent BV is associated with increased sPTB risk.