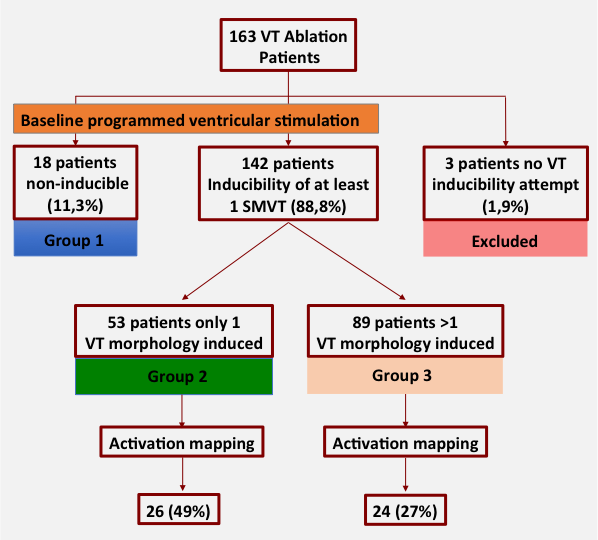
Introduction:Stand-alone substrate ablation without baseline ventricular tachycardia (VT) induction and activation mapping has become a standard VT ablation strategy. We sought to evaluate the influence of baseline VT inducibility and activation mapping on ablation outcomes in patients with structural heart disease (SHD) undergoing VT ablation. Methods:This is a single center, observational and retrospective study including consecutive patients with SHD and documented VT undergoing ablation. Baseline VT induction was attempted before ablation in all patients and VT activation mapping performed when possible. Ablation was guided by activation mapping for mappable VTs plus substrate ablation for all patients. Ablation outcomes and complications were evaluated. Results: 160 patients were included (203 VT ablation procedures) and were classified in 3 groups according to baseline VT inducibility: group 1 (non inducible, n=18), group 2 (1 VT morphology induced, n=53), and group 3 (>1VT morphology induced, n=89). VT activation mapping was possible in 35%. After a median follow-up of 38.5 months, baseline inducibility of >1VT morphology was associated with a significant incidence of VT recurrence (42% for group 3 vs. 15.1% for group 2 and 5.6% for group 1, Log-rank p<0.0001) and activation mapping with a lower rate of VT recurrence (24% vs. 36.3%, Log-rank p=0.035). Independent predictors of VT recurrences and mortality were baseline inducibility of >1VT morphology (HR 12.05 IC 95% 1.60-90.79, p=0.016) and LVEF<30% (HR 2.43 IC 95% 1.45-4.07, p=0.001), respectively. Complications occurred in 11.2% (5.6% hemodynamic decompensation). Conclusions:Baseline VT inducibility and activation mapping may add significant prognostic information during VT ablation procedur