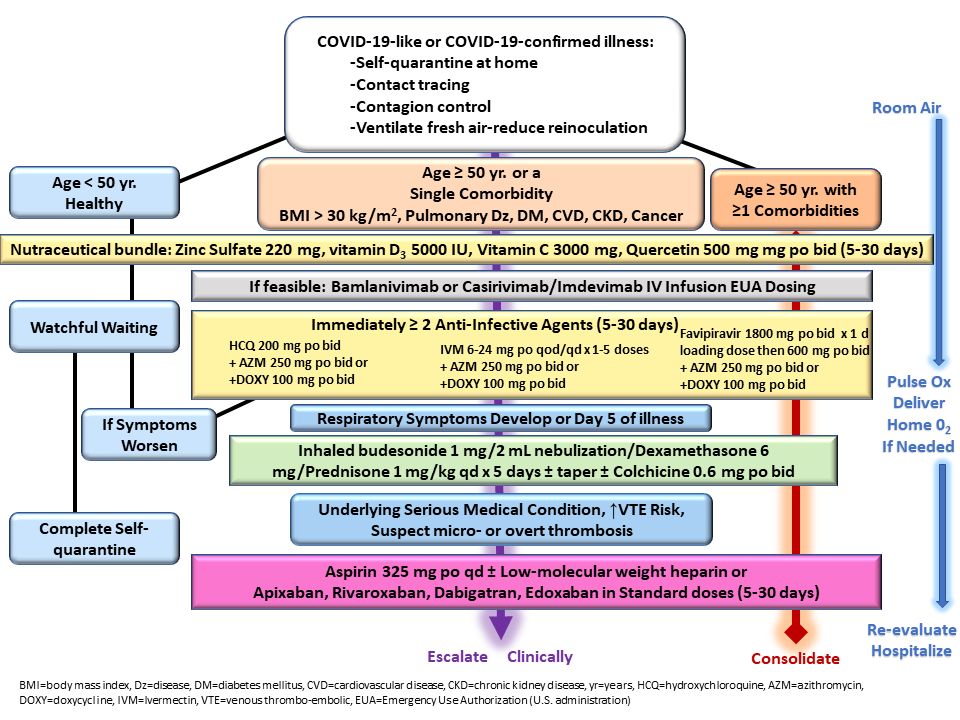
Background. There is an emergency need for early ambulatory treatment of COVID-19 in acutely ill patients in an attempt to reduce disease progression and the risks of hospitalization and death. Methods and Results. We recently reported results on 320 high-risk (age > 50 with ≥ 1 comorbidity) COVID-19 cases and have updated our results with 549 additional cases in period ending December 16, 2020. Our protocol utilizes at least two agents with antiviral activity against SARS-CoV-2 (zinc, hydroxychloroquine, ivermectin) and one antibiotic (azithromycin, doxycycline, ceftriaxone) along with inhaled budesonide and/or intramuscular dexamethasone. Albuterol nebulizer, inhaled budesonide, intravenous volume expansion with supplemental parenteral thiamine 500 mg, magnesium sulfate 4 grams, folic acid 1 gram, vitamin B12 1 mg, are administered for severely ill patients who either present or return to the clinic with severe symptoms. In period 1 (April-September, 2020) 6/320 (1.9%) and 1/320 (0.3%) patients were hospitalized and died, respectively. In period 2, (September-December, 2020) 14/549 (2.6%) and 1/549 (0.18%) were hospitalized and died, respectively. For comparison, we used the Cleveland Clinic COVID-19 hospitalization calculator and based on average age and comorbidities the expected rate of hospitalization for both periods was 18.5%. The cumulative mortality among confirmed and suspected COVID-19 in Collin, Dallas, Denton, and Tarrant counties was 0.76, 1.04, 0.90, and 0.97. As a result, our early ambulatory treatment regimen was associated with estimated 87.6% and 74.9% reductions in hospitalization and death respectively, p<0.0001. Conclusions. We conclude that early ambulatory, multidrug therapy is associated with substantial reductions in hospitalization and death compared to available rates in the community. Prompt ambulatory treatment should be offered to high-risk patients with COVID-19 instead of watchful watching and late-stage hospitalization for salvage therapies.