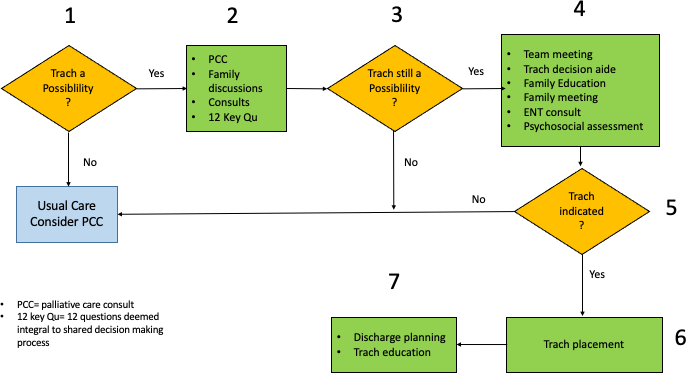
Background and objectives: Shared decision making (SDM) prior to non-urgent tracheostomy in a child with chronic respiratory failure (CRF) is recognized as the standard of care, but has proven challenging to implement in practice. We hypothesize that utilization of the microsystem model for analysis of the complex ecosystem in which SDM occurs will yield insights that enable formation of a reproducible, measurable SDM process. Methods: Retrospective chart review of a case series of children with CRF in whom a SDM process was pursued. The process included a palliative care consult, a validated decision aid and 12 key questions designed to elucidate information integral to an informed decision. Investigators reviewed a single hospital admission for each child, focusing on the 3 core elements of a medical microsystem- the patient, the providers, and information. Results: 29 patients who met inclusion criteria ranged in age from 0 to 19 years (median 1.7) and remained in the hospital from 10 to 316 days (median 38). Patients were medically complex with multiple and varied respiratory diagnoses, multiple and varied comorbidities, and varying psychosocial environments. 14/29 children received tracheostomies. Each child encountered a mean of 6.2 medical specialties, 1.9 surgical specialties and 8.5 non-physician led services. Answers to 12 key questions were not documented systematically and often not found. Conclusion: A unique SDM microsystem is formed around each child but not optimally utilized. Explicit recognition of these microsystems would enable team formation and an SDM process comprised of measurable steps and communication patterns.