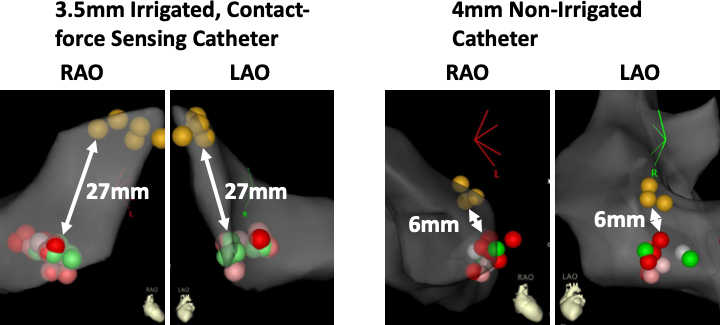
Introduction: Radiofrequency ablation (RFA) slow pathway modification for catheter ablation of AV nodal reentrant tachycardia (AVNRT) is traditionally performed using a 4mm, non-irrigated (NI) RF ablation catheter. Slow pathway modification using irrigated, contact-force sensing (ICFS) RFA catheters has been described in case reports, but outcomes have not been systematically evaluated. Methods: Acute procedural outcomes of 200 consecutive patients undergoing slow pathway modification for AVNRT were analyzed. An ICFS 3.5mm RFA catheter (ThermoCool SmartTouch STSF, Biosense Webster, Inc.) was utilized in 134 patients, and a 4mm NI RFA catheter (EZ Steer, Biosense Webster, Inc.) was utilized in 66 patients. Electroanatomic maps were retrospectively analyzed in a blinded fashion to determine proximity of ablation lesions to the His region. Results: Baseline characteristics of patients in both groups were similar. Total RF time was significantly lower in the ICFS group compared to the NI group (5.53±4.6 vs. 6.24±4.9 min, p=0.03). Median procedure time was similar in both groups, ICFS 108.0 (87.5-131.5) vs. NI 100.0 (85.0-125.0) min, p=0.2). Ablation was required in closer proximity to the His region in the NI group compared to the ICFS group (14.4 ± 5.9 mm vs, 16.7 ± 6.4 mm, respectively, p=0.01). AVNRT was rendered non-inducible in all patients, and there was no arrhythmia recurrence during follow-up in both groups. Catheter ablation was complicated by AV block in one patient in the NI group. Conclusion: Slow pathway modification for catheter ablation of AVNRT using an irrigated, contact-force sensing RFA catheter is feasible, safe, and may facilitate shorter duration ablation while avoiding ablation in close proximity to the His region.