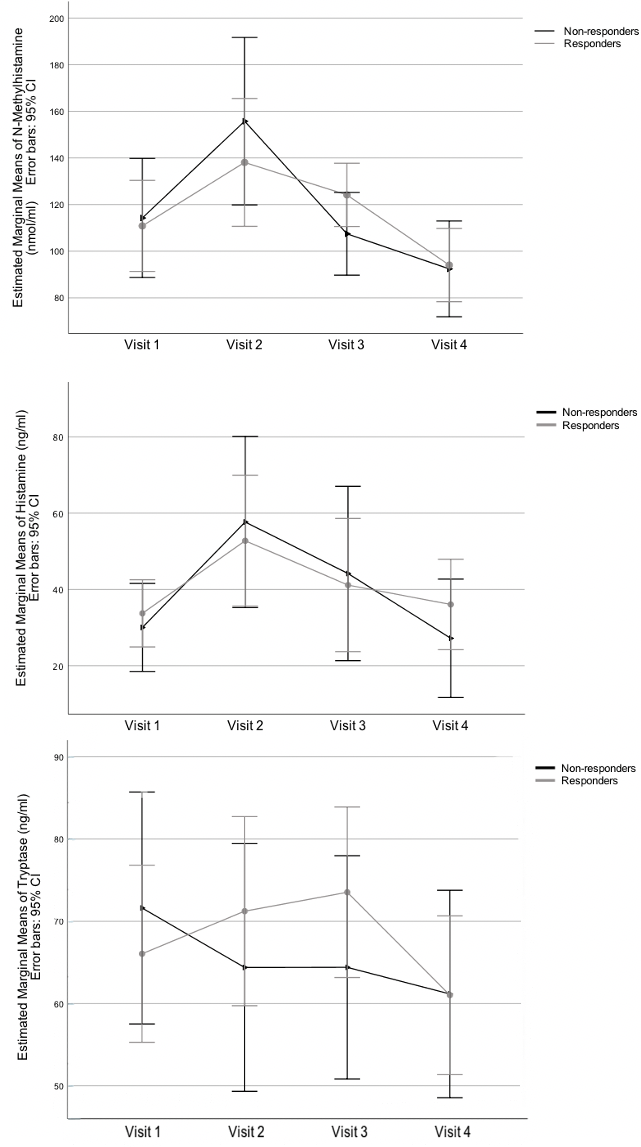
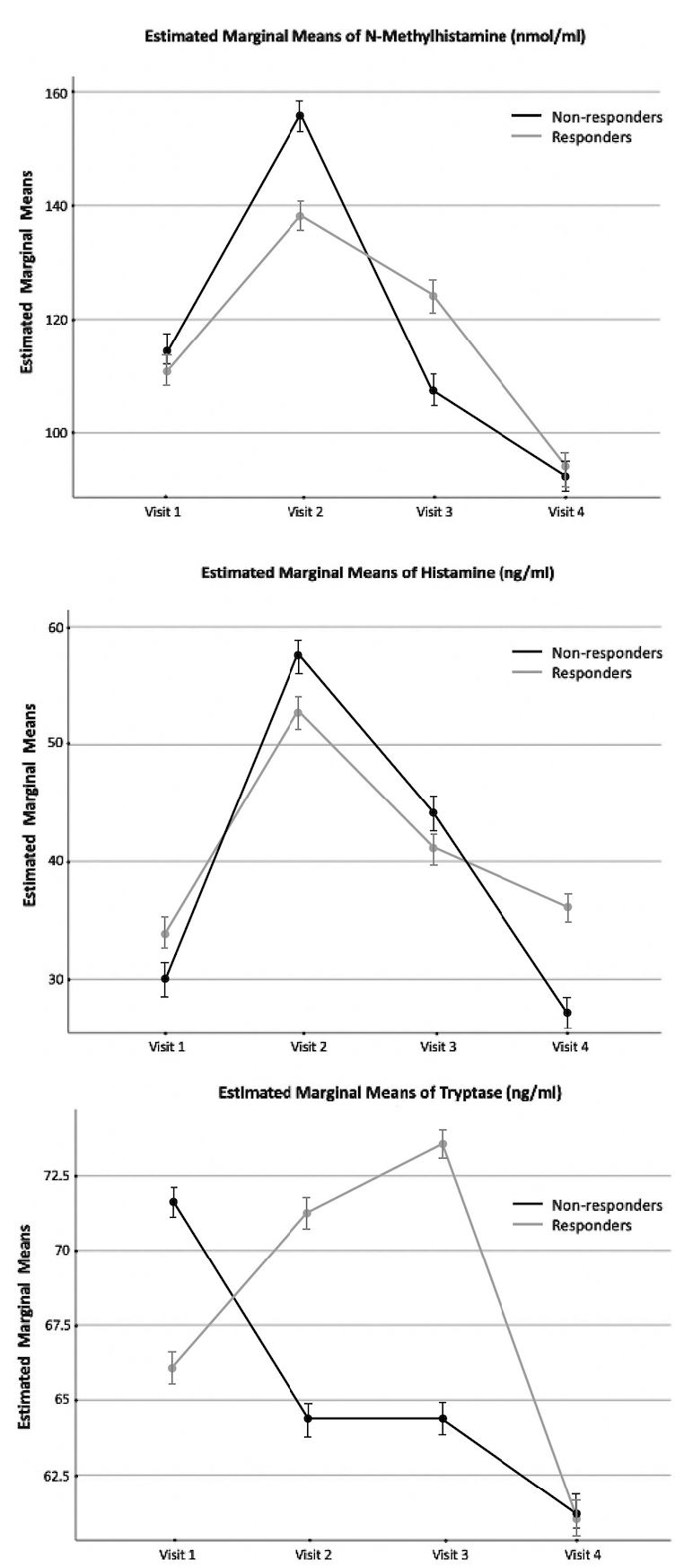
Background: Mast cells play a critical role in tumor-associated immune pathways. We aimed to determine whether the urinary mast cell mediators predict the immune response in patients with non-muscle invasive bladder cancer (NMIBC) treated with Bacillus Calmette-Guérin (BCG) immunotherapy. Methods: Nineteen patients who have received immunotherapy due to NMIBC and 19 healthy participants were enrolled. Urine samples were collected to assay N-methylhistamine, histamine, and tryptase levels immediately before the first BCG instillation, immediately after the third and sixth instillations, and four weeks after the sixth instillation in patients with NMIBC and at a single visit in healthy participants. Cystoscopic examinations were performed on the patient with NMIBC at three-month intervals for two years. The changes in urinary markers due to BCC response, BCG instillation, and the presence of NMIBC were assessed. Results: The average age was 56.1 ± 10.5 years in patients with NMIBC. Fourteen patients had high-grade Ta tumors, and 5 had high-grade T1 tumors. While 12 patients responded, 6 presented with recurrence and 1 with progression. There was no correlation between the levels of mast cell mediators and BCG response. The N-methylhistamine and histamine levels were increased significantly with the onset of immunotherapy, and N-methylhistamine levels were significantly decreased when immunotherapy was terminated. Pre-BCG estimated marginal means of N-methylhistamine were significantly higher in patients with NMIBC than healthy participants. Conclusions: Our study is the first study to identify the changes in mast cell mediators with the onset of immunotherapy and with the presence of bladder cancer. However, these mediators were not found to predict the patients’ response to immunotherapy.