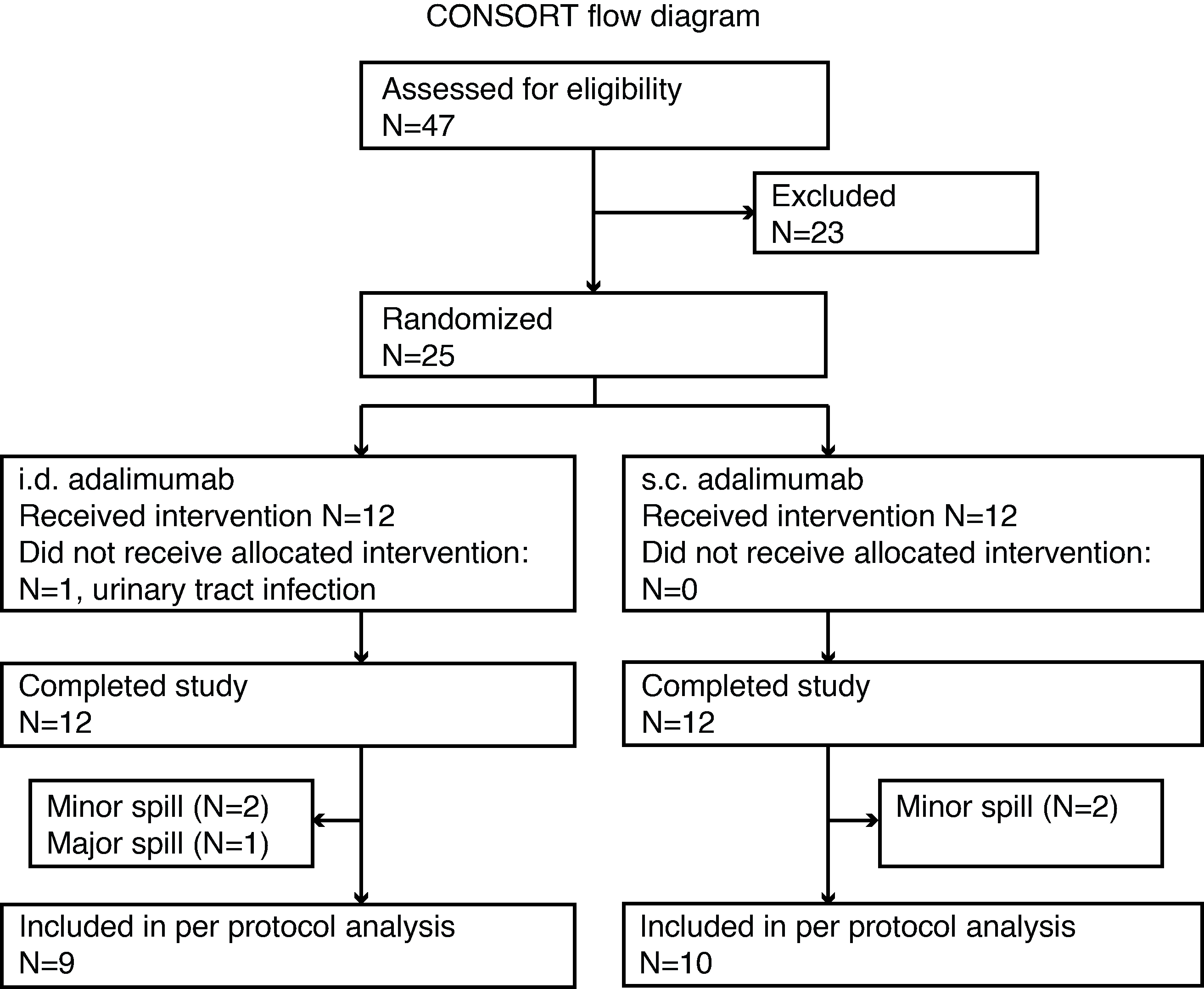
Aim To evaluate feasibility of intradermal (i.d.) adalimumab administration using hollow microneedles, and to compare a single i.d. dose of adalimumab using a hollow microneedle with a single subcutaneous (s.c.) dose using a conventional needle. Methods In this single-centre double-blind, placebo-controlled, double-dummy clinical trial in 24 healthy adults we compared 40 mg adalimumab (0.4 mL) administered i.d. using a hollow microneedle with a s.c. dose using a conventional needle. Primary parameters were pain, acceptability, and local tolerability; secondary parameters safety, pharmacokinetics and immunogenicity. We explored usability of optical coherence tomography (OCT), clinical photography, thermal imaging, and laser speckle contrast imaging (LSCI) to evaluate skin reaction after i.d. injections. In vitro protein analysis was performed to assess compatibility of adalimumab with the hollow microneedle device. Results While feasible and safe, injection pain of i.d. adalimumab was higher compared to s.c. adalimumab (35.4 vs. 7.9 on a 101-point VAS scale). Initial absorption rate and bioavailability were higher after i.d. adalimumab (Tmax=95h(47-120); F=129%(6.46%)) compared to s.c. adalimumab (Tmax=120h(96-221)). In 50% and 83% of the subjects anti-adalimumab antibodies were detected after i.d. and s.c. adalimumab, respectively. We observed statistically significantly more erythema and skin perfusion after i.d. adalimumab, compared to s.c. adalimumab and placebo injections (p<0.0001). Cytokine secretion after whole blood LPS challenge was comparable between administration routes. Conclusion Intradermal of adalimumab using hollowing microneedles was perceived as more painful, and less accepted than s.c. administration, however, yields a higher bioavailability with similar safety and pharmacodynamic effects.