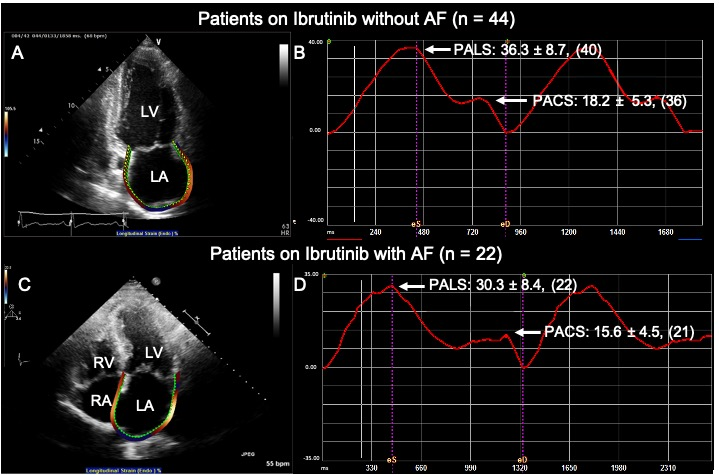
Background: Ibrutinib is associated with atrial fibrillation (AF), though echocardiographic predictors of AF have not been studied in this population. We sought to determine whether left atrial (LA) strain on transthoracic echocardiography could identify patients at risk for developing ibrutinib-related atrial fibrillation (IRAF). Methods: We performed a retrospective review of 66 patients who had an echocardiogram prior to ibrutinib treatment. LA strain was measured with TOMTEC Imaging Systems, obtaining peak atrial longitudinal strain (PALS) and peak atrial contraction strain (PACS) on 4-chamber and 2-chamber views. Statistical analysis was performed with Chi-square analysis, T-test, or binomial regression analysis, with a p-value < 0.05 considered statistically significant. Results: Twenty-two patients developed IRAF (33%). Age at initiation of ibrutinib was significantly associated with IRAF (65.1 years vs. 74.1 years, p = 0.002). Mean ibrutinib dose was lower among patients who developed IRAF (388.2 ± 121.7 vs. 448.6 ± 88.4, p = 0.025). E/e’ was significantly higher among patients who developed IRAF (11.5 vs. 9.3, p = 0.04). PALS was significantly lower in patients who developed AF (30.3% vs. 36.3%, p = 0.01). On multivariate regression analysis, age, PALS and PACS were significantly associated with IRAF. On multivariate regression analysis, only PACS remained significantly associated with IRAF while accounting for age. Conclusions: Age, ibrutinib dose, E/e’, and PALS on pre-treatment echocardiogram were significantly associated with development of IRAF. On multivariate regression analyses, age, PALS and PACS remained significantly associated with IRAF. Impaired LA mechanics add to the assessment of patients at risk for IRAF