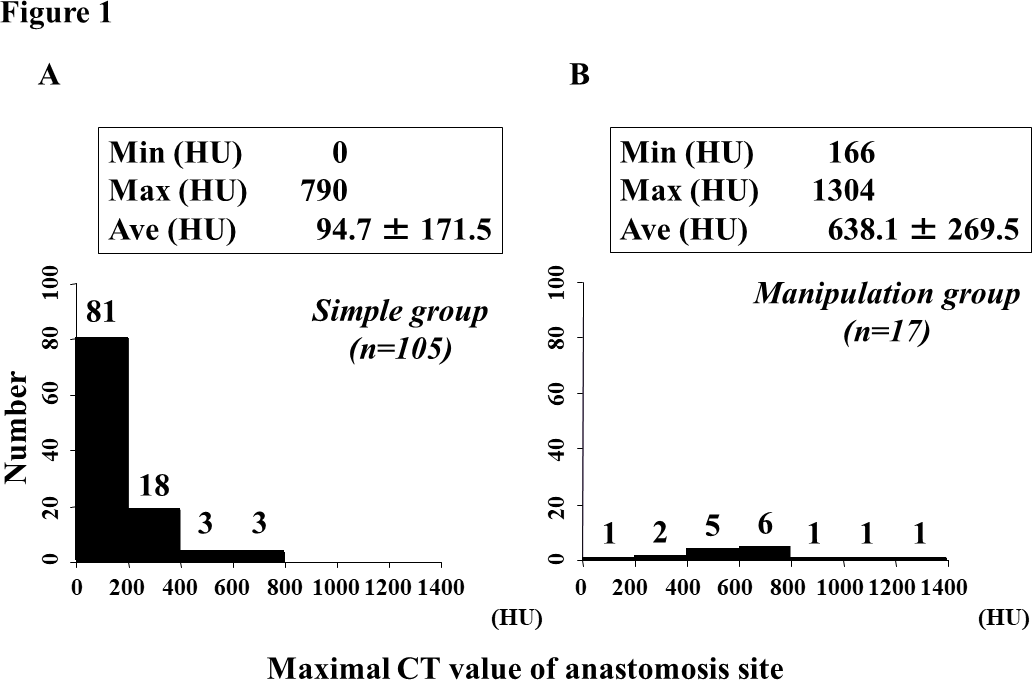
Background: Computed tomography (CT) is a useful tool for the identification of calcified lesions in the aorta. However, no quantitative evaluation has been established to assess the applicability of simple anastomosis preoperatively. We conducted this retrospective study to establish a reference range of the maximal CT value for application of simple anastomosis. Methods: 122 consecutive patients underwent replacement of the thoracic aorta between 2007-2011, excluding those with acute aortic dissection. The patients were divided into two groups: those who could undergo simple anastomosis (Simple group:n=105), and those who required endarterectomy prior to anastomosis (Manipulation group:n=17). The maximal CT value at the anastomosis site was calculated by an imaging software. Results: The mean maximal CT value (Hounsfield unit: HU) was significantly higher in the Manipulation group (638.1 ± 269.5 [166-1304]) than in the Simple group (94.7 ± 171.5 [0-790]) (p<0.0001). The maximal CT value enabled us to predict the simple anastomosis with the area under the receiver operating characteristic curve of 0.96 (p<0.0001). The cut-off value was 325 HU (sensitivity 94.1%, specificity 81.7%). The 10-year survival rate was significant lower in the Manupilation group (11.8%) than in the Simple group (43.2%). In the multivariate analysis, age (Hazard Ratio [HR]:1.073), Hypertension (HR:2.382) and maximal CT value (HR:1.001) were independently associated with long-term mortality. Conclusions: Preoperative evaluation of the maximal CT value is a useful tool in predicting whether simple anastomosis is applicable or not, in the thoracic aortic surgery. Maximal CT value is a risk factor for long-term mortality.