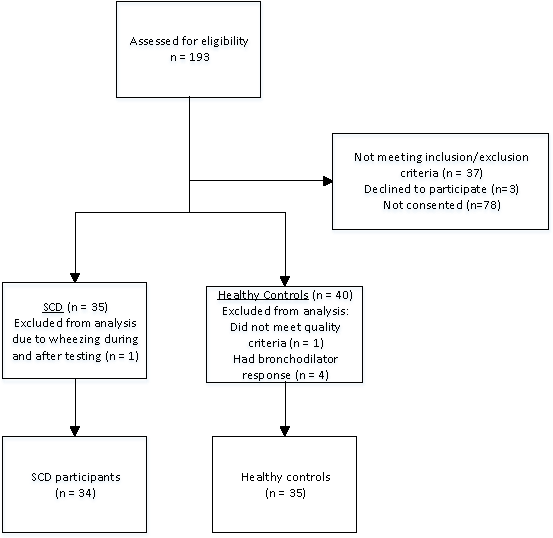
Introduction: The Lung Clearance Index (LCI) derived from the multiple-breath washout test (MBW), is both feasible and sensitive to early lung disease detection in young children with cystic fibrosis and asthma. The utility of LCI has not been studied in children with sickle cell disease (SCD). We hypothesized that children with SCD, with or without asthma or airway hyper reactivity (AHR), would have an elevated LCI compared to healthy controls. Methods: Children with SCD from a single center between the ages of 6-18 years were studied at baseline health and completed MBW, spirometry, plethysmography and blood draws for serum markers. Results were compared to healthy controls of similar race, age and gender. Results: Control subjects (n=35) had a significantly higher daytime oxygen saturation level, weight and body mass index (BMI) but not height compared to subjects with SCD (n=34). Total Lung Capacity(TLC) z-scores were significantly higher in the healthy controls compared to those with SCD (0.87 (1.13), 0.02 (1.27), p=0.005) while differences in Forced Expiratory Volume in 1 second (FEV1) z-scores approached significance (0.26 (0.97), -0.22 (1.09), p=0.055). There was no significant difference in LCI among the comparison groups (7.29 (0.72), 7.40 (0.69), p=0.514). Conclusion: LCI did not differentiate SCD from healthy controls in children between the ages of 6 and 18 years at baseline health. TLC may be an important pulmonary function measure to follow longitudinally in the pediatric SCD population.