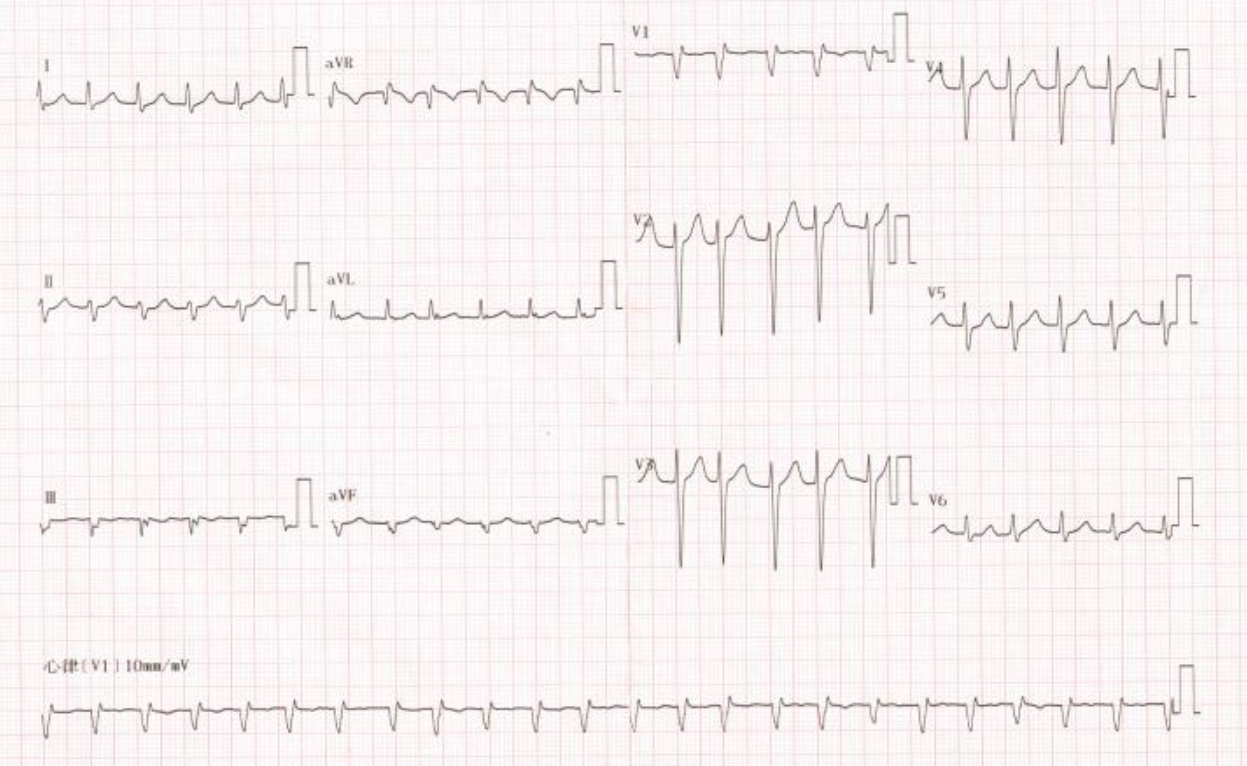
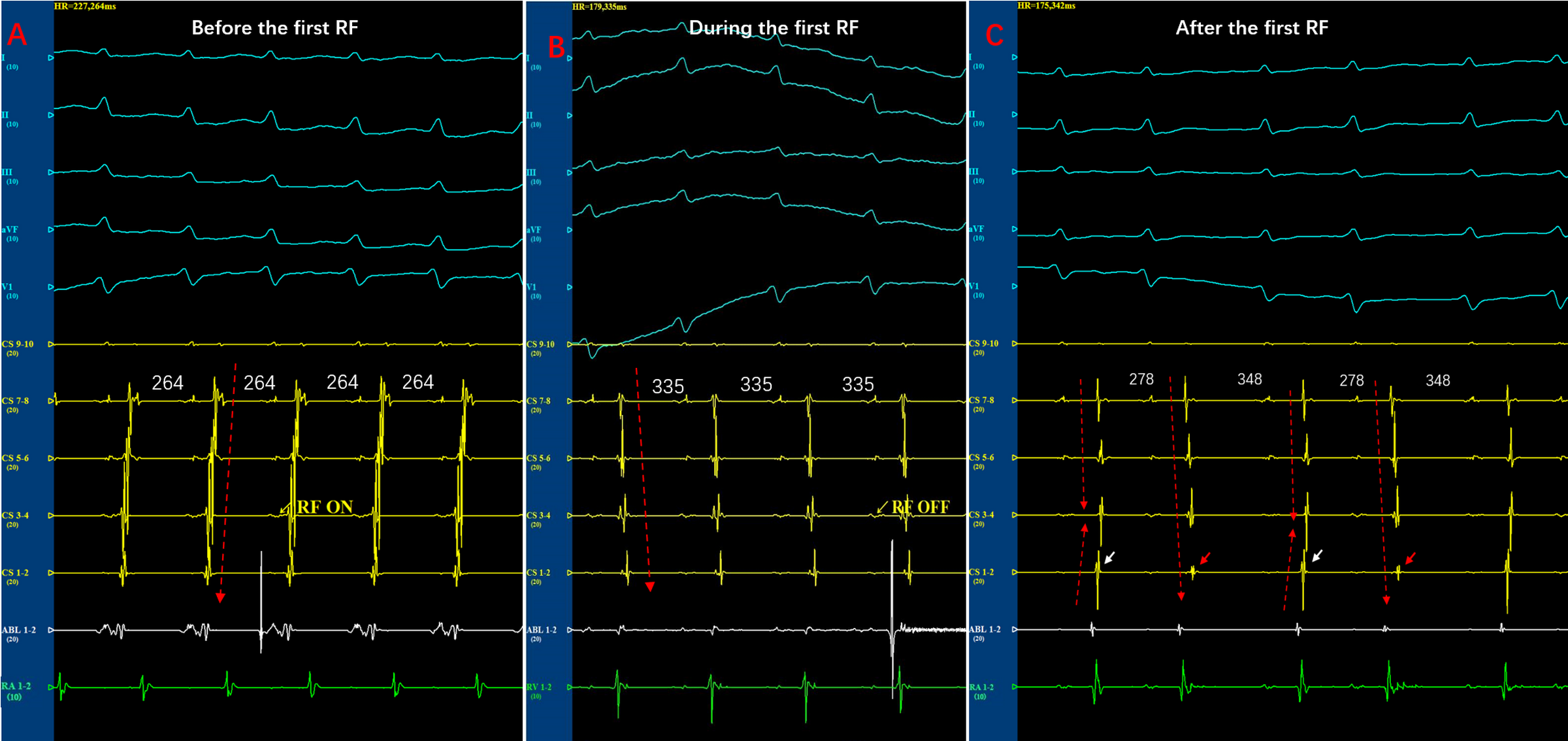
A narrow QRS complex tachycardia with irregular rhythm: what Is the mechanism?Liu Qifang MD, Tian Ye MD, Zhao Yidong MM, Yang Long MD.PHD,Department of Cardiology,Guizhou Provincial People’s Hospital, Guiyang , ChinaCorresponding anthor: Yang Long E-mail:[email protected]:(None)Funding: Clinical Research Center Project of Department of science and technology of guizhou province [NO. (2017)5405]Key Words: Atrioventricular nodal reentrant tachycardia;Catheter ablation;Irregular rhythmAbstractIn most patients with atrioventricular nodal reentrant tachycardia (AVNRT), mutiple slow pathways are involved in anterograde conduction,resulting in repetitive alternans or triplets in tachycardia cycle-length that display regularly irregular tachycardia. We describe a patient with AVNRT presenting completely irregular rhythm that may mimic atrial fibrillation. A single radiofrequency energy delivery in the posterior septum near the ostium of the coronary sinus effectively eliminated the tachycardia. The anisotropic conduction of the transitional area of the slow pathway can be responsible for anterograde AV node conduction intervals fluctuation and circle length variation.Case reportA 56-year-old man with a history of hypertension and recurrent palpitations was referred to our institution for electrophysiological examine. Physical examination, chest CT, and the baseline 12-lead electrocardiography (ECG) was normal. A 24-h Holter monitor did not record any arrhythmias. During the palpitation,the narrow QRS complex tachycardia with variable R-R intervals was recorded on surface electrocardiogram(figure 1). This irregular narrow QRS complex tachycardia could be misinterpreted as multifocal atrial tachycardias or atrial fibrillation because varying RR intervals [1]. During the electrophysiological study, intracardiac electrograms revealed normal A-H interval 80ms and H-V interval of 45ms in sinus rhythm. Ventricular overdrive pacing at a cycle length of 400ms resulted in ventriculoatrial dissociation. Atrial programmed stimulation was introduced during sinus rhythm with a cycle length of 500 ms and the coupling interval was reduced from 420 to 300 ms(-10ms decrease).The A2 to V2 conduction curves were continuity and there was no a jump(>50 ms) at a critical range of A1 to A2 coupling intervals,indicating dual pathway physiology of AV node was not found in this case(figure 2)[2].An irregular, sustained, narrow-QRS complex tachycardia was induced by atrial overdrive stimulation with a cycle length of 280 ms,The atrial activation sequence during the tachycardia is concentric and atrial and ventricular activation are simultaneous(figure 3). Overdrive ventricular stimulations during tachycardia did not affect the activation sequence of atria and there was no regular relation between ventricular and atrial activations. The diagnosis of atrioventricular reciprocating tachycardia was excluded. The premature atrial impulses were introduced with different coupling intervals,the His-atrial interval of the return cycle still remained constant. The diagnosis of atrial tachycardia is unlikely, AVNRT is by far the most likely mechanism. Interestingly,there were large fluctuations in the AH interval and HV interval remained constant during tachycardia(figure 4). What is the mechanism for the AH interval fluctuation and irregular rhythm?DISCUSSIONIn this case. we reported a patient with AVNRT showing irregular rhythm and the large fluctuations in AH interval during the tachycardia. There are two reasons for the cycle length and A-H intervals beat to beat variability in a patient with AVNRT:1)The spontaneous transition of multiple different reentry circuits using different anatomic slow pathways with alternans pattern to interact with the retrograde fast pathway[1]. 2)The anisotropic conduction of the transitional area of the slow pathway. In our patient,the dual pathway physiology of AV node was not found during electrophysiologic study, indicating the absence of multiple anatomic slow pathway available for anterograde conduction. Furthermore, a single radiofrequency delivery in the posterior septum near the ostium of the coronary sinus effectively eliminated the tachycardia. If one cannot exclude the possibility of two or three anatomically distinct slow pathways with closely spaced insertion sites, it is possible to eliminate two or three antegrade slow pathways conduction by a single ablation lesion in posteroseptal region [2]. However, our patient exhibited too many AH conduction intervals during the tachycardia. therefore, we could not simultaneously eliminate all slow pathway with different anatomic distinction by a single lesion at the right posterior atrial septum. Therefore, these findings imply that anisotropic conduction of slow pathway with a single anatomic localization are more likely to be responsible for the tachycardia cycle length variety in this patient.In 1998, Becker demonstrated the presence of the inferior extensions of the AV node in the human heart. AVNRT is defined as a re-entrant tachycardia utilizing the AV node and the right and left inferior extensions as the substrate of their circuit. Recently, Anderson identified ubiquitous connections between the working myocardium of the atrial septum and the compact node through transitional cells. These anatomic features could provide an electrophysiological substrate for the development of irregular rhythm in our patient [3]. Circle lengths variation or AH intervals fluctuation result from spontaneous transition from one to another permutation of the different fast pathway and slow pathway [4]. However,It is impossible that the transition of different reentrant circuits can be responsible for cycle length variation,because the conduction properties of all slow pathways are not appropriate to simultaneously interact with the retrograde fast pathway in an episode of tachycardia. The reasonable explanation for this phenomenon is that the conduction velocity differences in slow pathway based on nonuniform anisotropy may form the irregular tachycardia substrate in our patient [5].The right inferior input has a higher Cx43 expression than the node itself, which provided histologic and electrophysiologic evidence for the anisotropic conduction of the transitional area of the AV node [6]. In our patients, the variability in the space construction of the AV node and the differential expression of connexin isoforms in the nodal area may be responsible for diversity conduction characteristics of slow pathways.Conference[1] Richter S, Berruezo A, Mont L, Boussy T, Sarkozy A, Brugada P, Brugada J. Pseudo–Atrial Fibrillation, Rare Manifestation of Multiple Anterograde Atrioventricular Nodal Pathways. Am J Cardiol 2007;100:154 –156.[2] Tai CT, Chen SA, Chiang CE, Lee SH, Chiou CW, Ueng KC, Wen ZC, Chen YJ, Chang MS. Multiple anterograde atrioventricular node pathways in patients with atrioventricular node reentrant tachycardia. J Am Coll Cardiol 1996;28(3):725-731.[3] Anderson RH, Sanchez-Quintana D, Mori S, Cabrera JA, Back Sternick E. Re-evaluation of the structure of the atrioventricular node and its connections with the atrium. Europace 2020 May 1;22(5):821-830.[4] Katritsis DG, Camm AJ. Atrioventricular nodal reentrant tachycardia. Circulation. 2010 ;122(8):831-40.[5] Katritsis DG. A unified theory for the circuit of atrioventricular nodal re-entrant tachycardia. Europace. 2020 ;22(12):1763-1767.[6] Katritsis DG, Efimov IR. Cardiac connexin genotyping for identification of the circuit of atrioventricular nodal re-entrant tachycardia. Europace 2019 ;21(2):190-191.Lengend:Figure 1 The narrow QRS complex tachycardia with a completely irregular rhythm.Figure 2 There is no jump in A2-V2 interval at a critical range of A1-A2 coupling intervals.Figure 3 Intracardiac recordings during tachycardia showing tachycardia cycle length variation.Figure 4 Intracardiac recordings during tachycardia showing the fluctuation of A-H intervals and constant of H-A intervals.