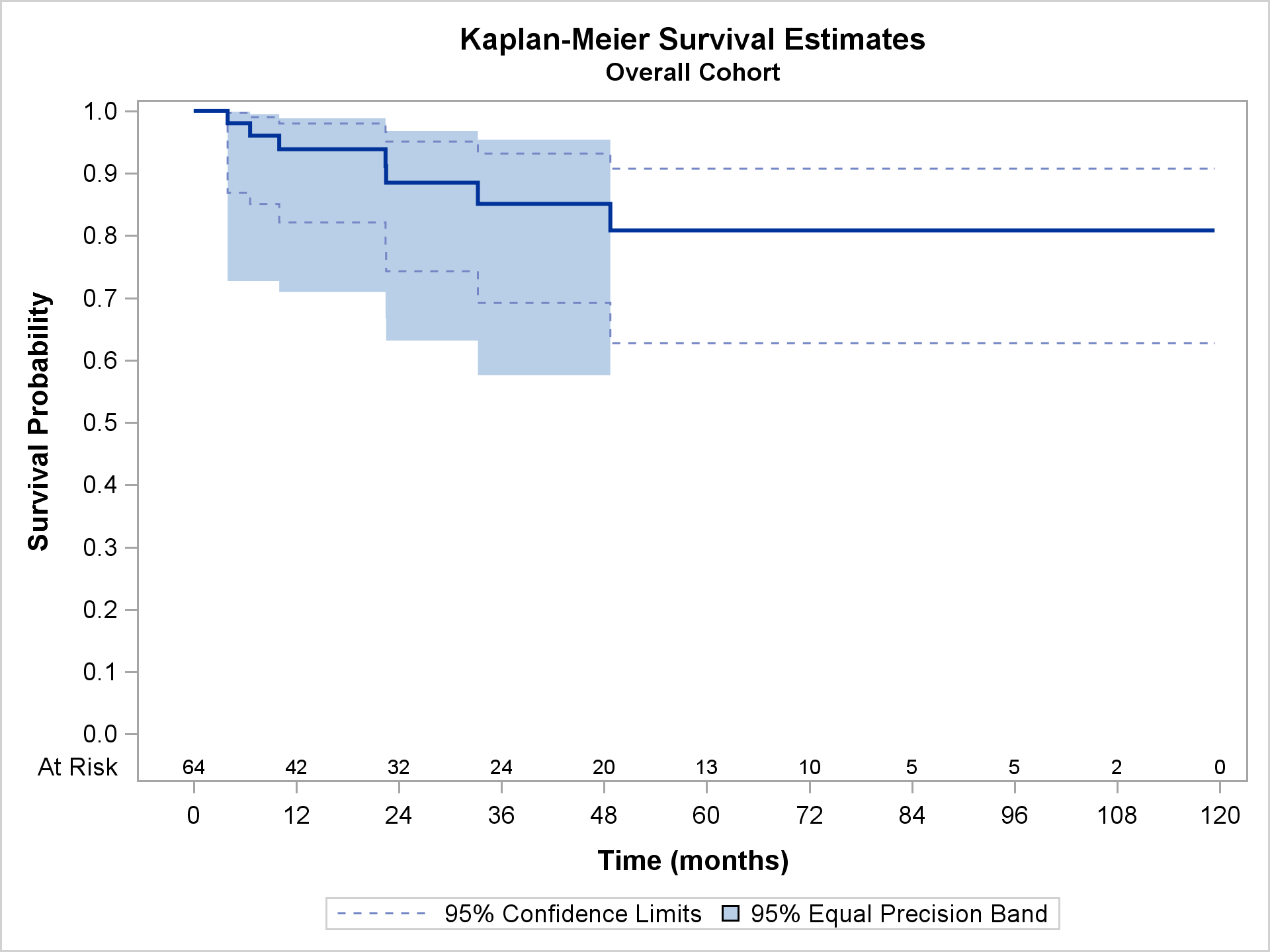
Objectives: To compare outcomes after the development of early (≤30 days) versus delayed (>30 days) deep sternal wound infection (DSWI) after cardiac surgery. Methods: Between 2005 and 2016, 64 patients were treated surgically for DSWI following cardiac surgery. Thirty-three developed early DSWI, while 31 developed late DSWI. Mean follow up was 34.1 ± 32.3 months. Results: Survival for the entire cohort at 1, 3, and 5 years was 93.9, 85.1, and 80.8%, respectively. DSWI diagnosed early and attempted medical management were strongly associated with overall mortality (hazard ratio (HR), 25.0 and 9.9; 95% confidence intervals (CI), 1.18-528 and 1.28-76.5; p-value 0.04 and 0.04, respectively). Survival was 88.1, 77.0, 70.6 and 100, 94.0 and 94.0% at 1,3, and 5 years in the early and late DSWI groups, respectively (Log-rank = 0.074). Those diagnosed early were more likely to have a positive wound culture (odds ratio (OR), 0.06, 95% CI 0.01-0.69, p=0.024) and diagnosed late were more likely to be female (OR 8.75, 95% CI 2.0-38.4, p=0.004) and require an urgent DSWI procedure (OR 9.25, 95% CI 1.86-45.9, p=0.007). Both early diagnosis of DSWI and initial attempted medial management were strongly associated with mortality (hazard ratio 7.48, 95% CI 1.38-40.4, p=0.019 and hazard ratio 7.76, 95% CI 1.67-35.9, p=0.009, respectively). Conclusions: Early aggressive surgical therapy for deep sternal wound infection after cardiac surgery results in excellent outcomes. Those diagnosed with DSWI early and have failed initial medical management have increased mortality.