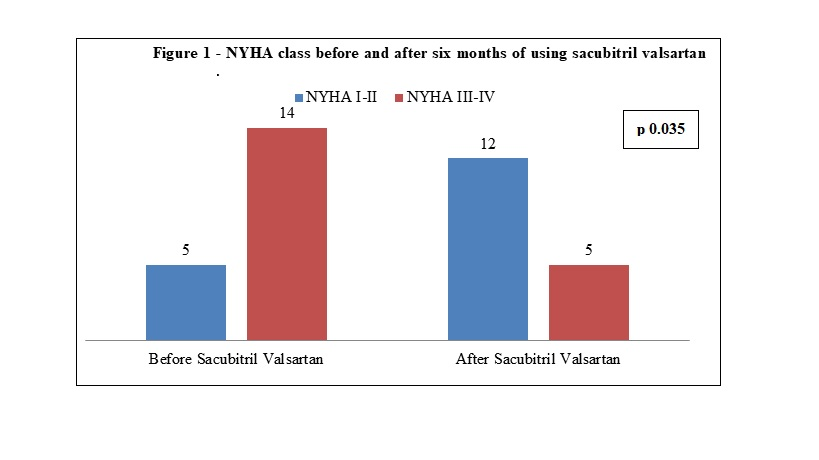
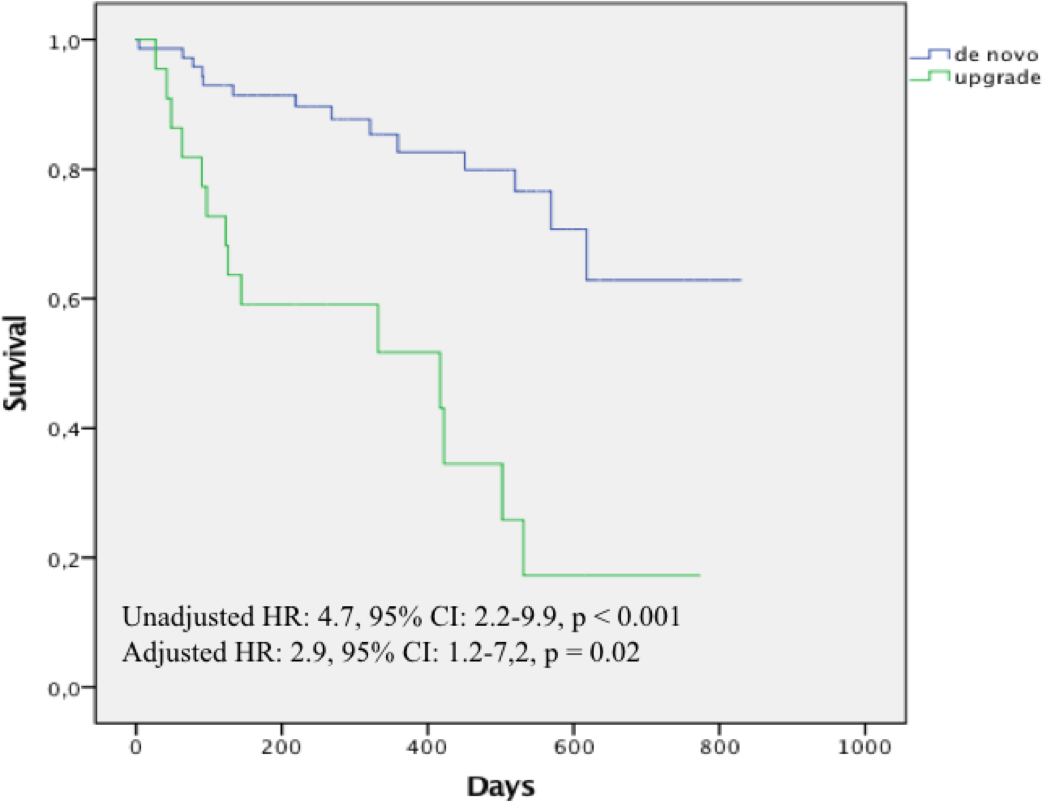
Introduction: Cardiac resynchronization therapy (CRT) improves outcomes in heart failure (HF) patients with left bundle branch block (LBBB). However, the benefits of CRT in patients with previous pacing are uncertain, specially in a population witch Chagas disease is a prevalent cause of HF. Methods and Results: Prospective cohort study that included HF patients indicated for CRT with left ventricular ejection fraction (LVEF) of less than 35%. Clinical and demographic data were collected to investigate mortality predictors after 1 year. The overall survival was calculated by the Kaplan-Meier method and multivariate analysis using Cox’s regression model was performed. Between May 2017 and September 2019, 93 patients were evaluated with a mean follow-up of 1,0 (0.6) year. Of these, 22 (23,7%) were upgraded from right ventricular pacing. Chagas Disease was the most prevalent cause of HF 29 (31,2%). In overall patients, LVEF at 6 months increased after CRT: 24,0% (7,8) to 30,3% (11,5), p=0.007, and there was no significant difference between upgraded patients and de Novo CRT, p=0.26. Overall mortality at 1-year was 28 (30,1%). In the univariate analysis, Chagas disease and upgraded therapy were associated with mortality at follow-up, HR: 3.9, CI: 1.8-8,4, p = 0.001 and HR: 4.7, CI: 2.2-9.9, p < 0.001, respectively. In the multivariate model, only upgraded therapy remained independently associated with the outcome, adjusted HR: 2.9, CI: 1.2-7,2, p = 0.02. Conclusion: In this specific HF population, with a high prevalence of Chagas disease cardiomyopathy, upgraded therapy was independently associated with worsened 1-year survival after CRT.