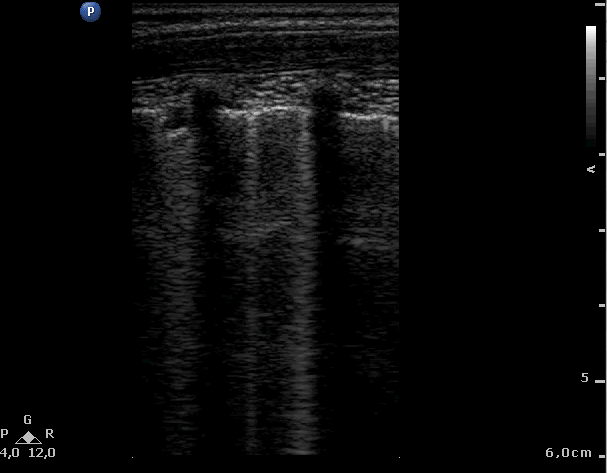
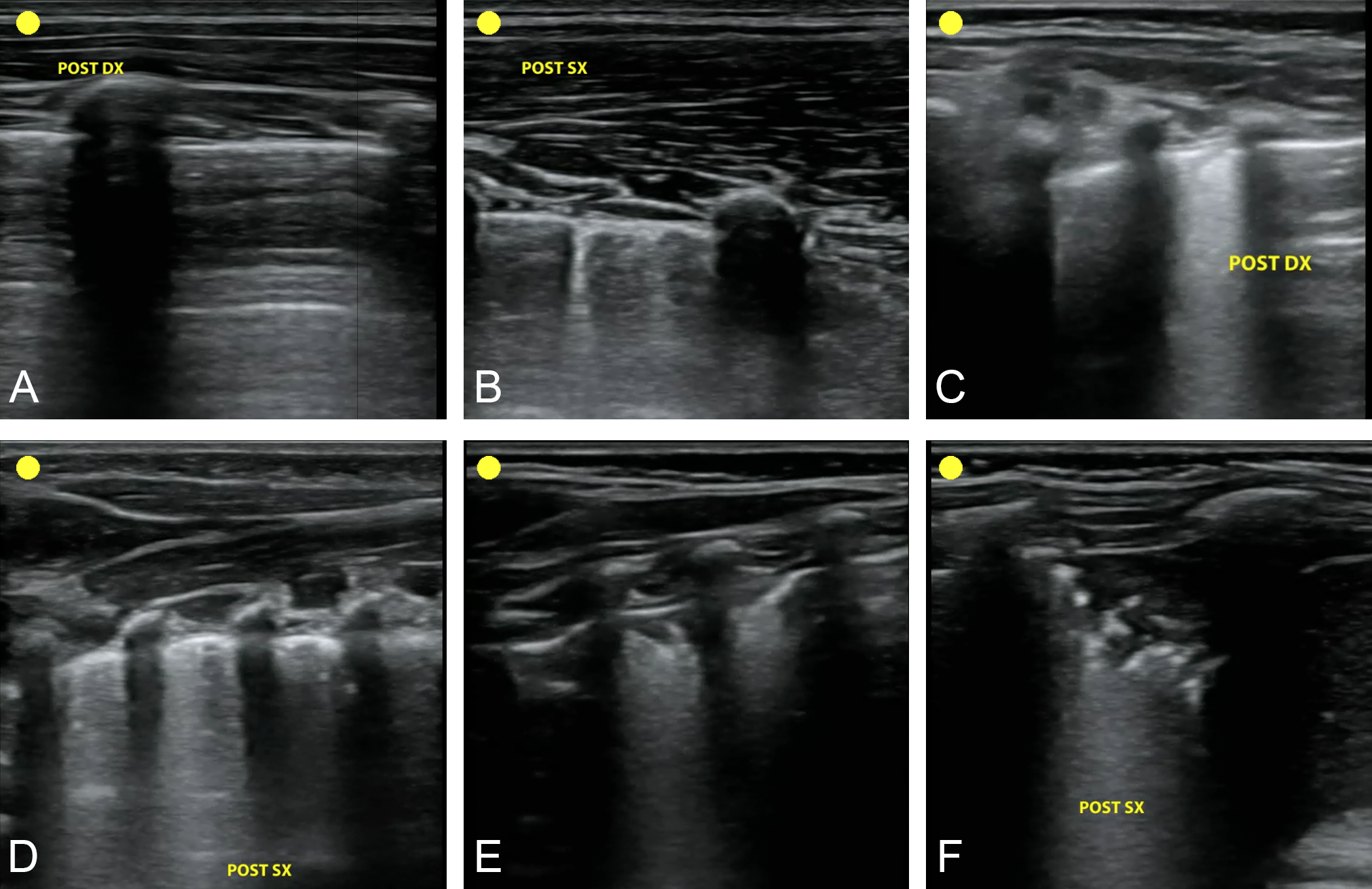
The evaluation of the lung by ultrasound is an adjunct tool to the clinical assessment. Among different hallmarks at lung ultrasound, B-lines are well known artifacts which are not correlated to identifiable structures but can be used as an instrument for pathological classification. Multiple B-lines are the sonographic sign of lung interstitial syndrome with a direct correlation between the number of B-lines and the severity of the interstitial involvement of lung disease. In neonatology and paediatrics, the quantitative assessment of B-lines is questionable as opposed to in adult medical care. Counting B-lines is an attempt to enrich the clinical assessment and clinical information, and not simply arrive at a dichotomous answer. A semiquantitative or quantitative B-lines assessment was shown to correlate with fluid overload and demonstrated prognostic implications in specific neonatal and paediatric conditions. In neonatology, the count of B-lines is used to predict the need for admission in neonatal intensive care unit and the need for exogenous surfactant treatment. In paediatrics, the B-lines count has the role of quantifying hypervolemia in infants and children receiving dialysis. B-lines as predictors of length of stay in the paediatric intensive care unit after cardiac surgery, as a marker of disease severity in bronchiolitis, or as an indicator of lung involvement from SARS-CoV-2 infection are speculative and not yet supported by solid evidence. Lung ultrasound with the quantitative B-lines assessment is promising. The current evidence allows to use the quantification of B-lines in a limited number of neonatal and paediatric diseases.