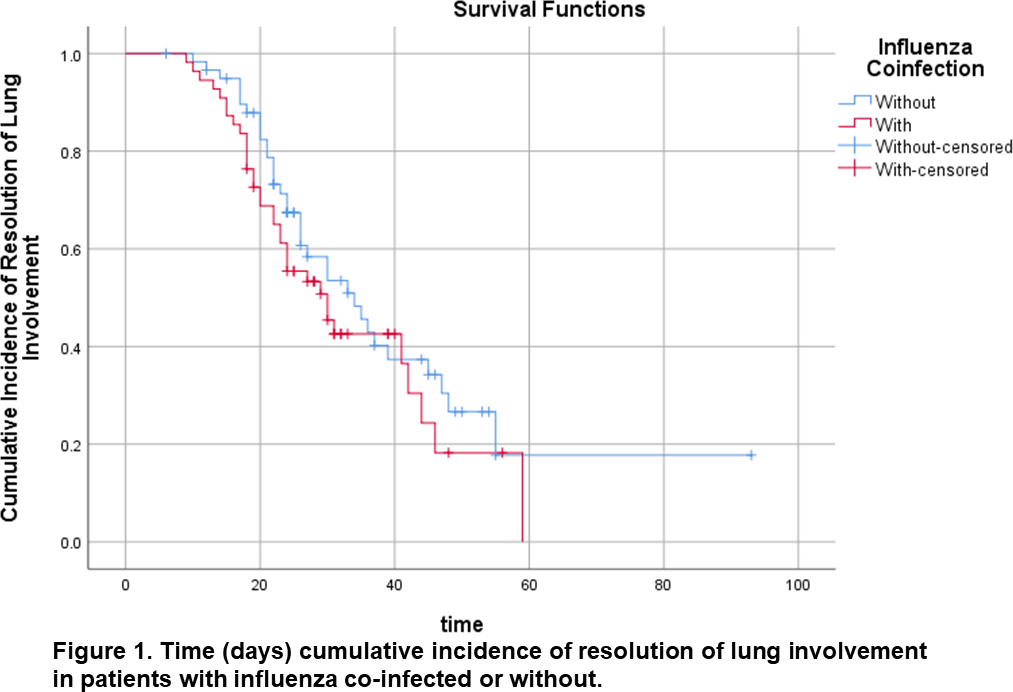
Background: Little is known about whether coinfection of other respiratory tract viruses contributes to severity of COVID-19 pneumonia. Methods: We retrospectively studied 128 hospitalized patients with COVID-19 pneumonia (64 cases co-infected with influenza A/B vs 64 negative influenza cases via pair-matching on age, sex, and days from onset of symptom). Results: Among 64 co-infected patients, 54 patients (84.4%) had co-infected with influenza A, and 10 (15.6%) with influenza B. The percentages for the severity of pneumonia on admission of the two groups, i.e., with influenza infection and without, were similar (P=0.945). The median duration (days) of viral shedding time from admission was longer for patients with influenza infection (17.0 day) than those without influenza infection (12.0 day) (P<0.001). However, the progression of lung CT in four weeks after onset of symptom were similar in both groups. The multivariable Cox proportional hazards model showed that the HR of pneumonia resolution on CT scans was 0.869 (P=0.612) for patients with influenza (95% CI 0.505, 1.495) compared with patients without influenza, while the HR of resolution in lung involvement was 1.878 (P=0.020) for patients with lopinavir/ritonavir, compared with patients without lopinavir/ritonavir (95% CI 1.103, 3.196). Patients who were treated with lopinavir/ritonavir presented with faster pneumonia resolution in two weeks after symptom onset both in the whole cohort (32.4% vs 13.8%, P=0.036) and in influenza co-infected group (37% vs 1%, P=0.001). Conclusions: Lopinavir/ritonavir eliminated the difference of lung involvement between influenza co-infected and non-infected groups, indicating lopinavir/ritonavir is associated with pneumonia resolution in COVID-19.