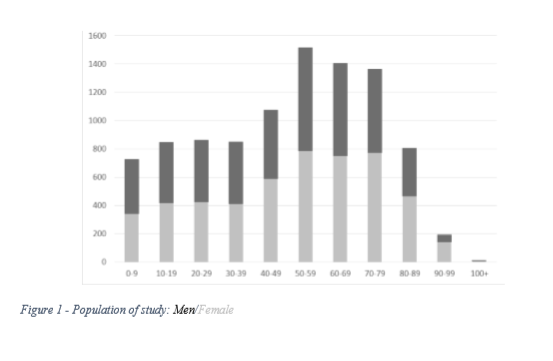
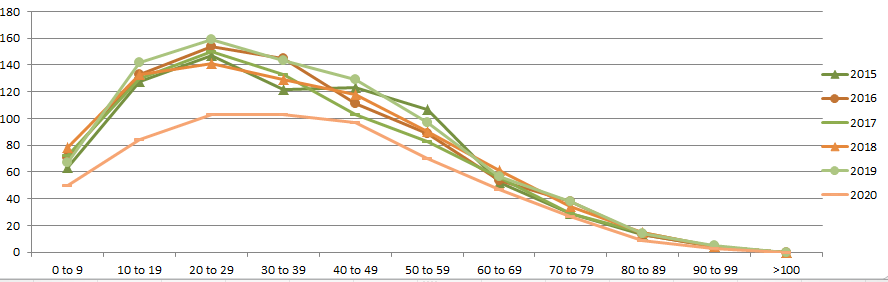
Introduction In different Countries and different Healthcare Systems, GP workload is significantly burdened by a minority of patients seeing their GP a lot more often than their peers (1).Those are patients are generally well-known to their family physician as subjects that make the ”heart sink” and therefore were initially called by O’Dowd “heartsink patients” (2).But when, more precisely, a patient “becomes” a high user or frequent attender ”?Even if the phenomenon is not new, we do not have data to define quantitatively this “entity” and we ignore if the prevalence of FAs as increased over time, or if it hasn’t (3,4).We do not have precise data about the average duration of their GP encounters, which could well differ from the standards 10 minutes, hence likewise affecting the burden on GP time.To describe those patients, we still often reference to a work published in 1988. It is believed that Tom O’Dowd then coined the term ”heartsink”, to describe ”The feeling experienced (by the family doctor) when their names (of patients) appear in the list of the morning appointments. ” (1)Further work has been done to define the reasons behind the frequent GP visits. In 1988, O’Dowd acknowledged that the medical experience was subjective, but perceived that the problem and its solution resided both in the patient.A systematic review from Gill and Sharpe on prevalence, associations and clinical outcomes, and subsequent observations from other Authors, have shown that FAs have high rates of physical illnesses, psychiatric illnesses, social difficulties and emotional distress (3,5).Frequent attendance in General Practice is also considered an indicator of behaviour of inappropriate use of other health services, in particular emergency departments and Secondary Care services (6,7,8).Evidence of the effect of (mainly psychiatric) interventions on the rate of frequency and morbidity ofFAs have shown conflicting results (9,10). In a review of the interventions on FAs, it was found thatthe high frequency can be a sign of a major depressive disorder and that its treatment can improve the depressive symptoms, but there is no evidence that it is thereby possible to influence the use of the services (11).The interpretation of the studies on FAs is hampered by differences in Healthcare Systems and in the definition of FA (12).It has been shown that age and sex are highly associated to the number of GP visits and that the identification of FAs without adjustment by age and sex leads predominantly to the selection of older women (13).After reviewing the literature on high users, Vedsted suggested that the FA should be described as a subject that falls at the top 10% of the practice population stratified by age and gender (4).Vedsted, suggested to arbitrarily fix a threshold in the distribution of the frequency of consultation, such that they are considered FAs all those who go above the percentage or percentile set as threshold.However, this choice is associated with various problems of practicality with one key disadvantage that is of failing to identify a number of variabilities in relation Health Care System, for instances.In this work, we checked the frequency GP encounters, both in office and at patient’s domicile, over the course of 12 months, in both sexes, and in all age bands.We then looked at the number of visits over the course of a year above which such number increases rapidly, isolating a limited group of patients to whom was associated an extremely high number of GP encounters.Doing so, we aimed to clarify if and where the proportional threshold value and the absolute threshold value may converge.We believe that they do converge and that this number can be identified as the most useful threshold value for the definition FA.MethodIn the context of a General Practice medium density urban setting, we collected data on 9651 people registered with 4 different GPs.Unlike most previous studies on FAs, we have not ruled out children and the most elderly.In fact, several studies have only used data from patients aged 15 to 74 years.For all patients registered during the 12 months prior to the audit date, we only counted the GP face to face consultations, either at the Surgery or at home of the patient. We have calculated the contact frequencies of all patients for each combination of age and gender. The top 5% of patients in terms of frequency of yearly encounters has been defined using the concept of proportional threshold.ResultsThe characteristics of the population studied is graphically represented in figure 1, they are the following:Mother population: Patients currently registeredLast Search: 01-mar-2018Relative Date: 01-Mar-2018Population count: 9651Males: 4540Females: 5111