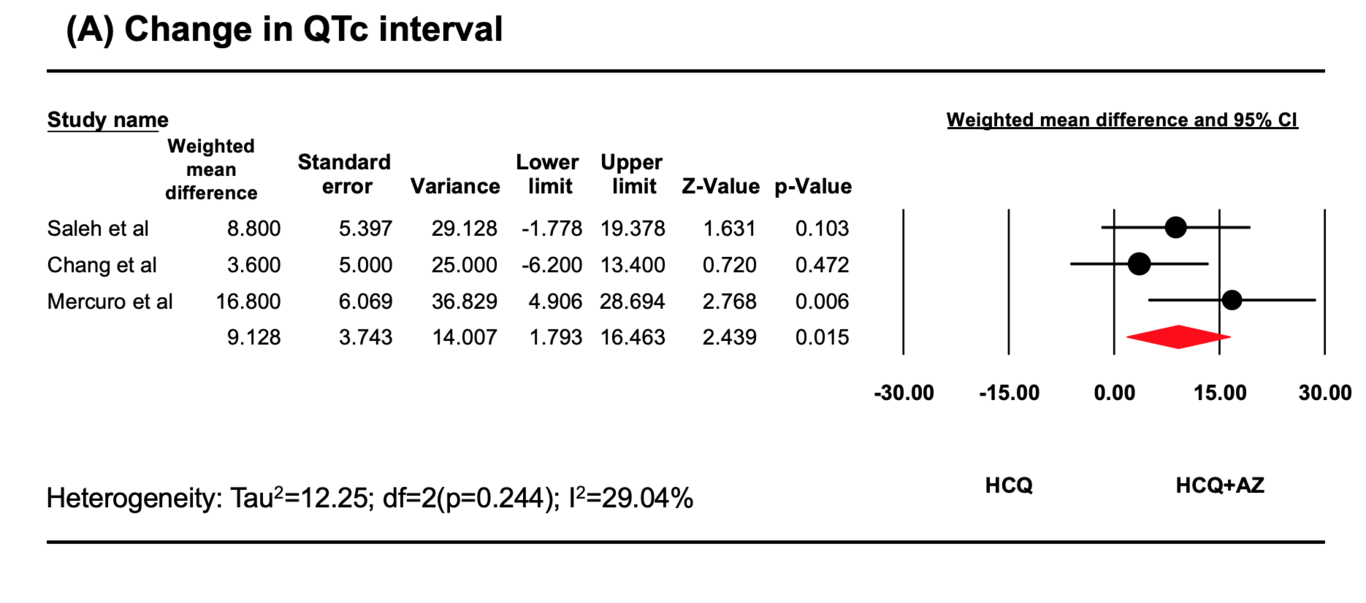
Introduction: Hydroxychloroquine (HCQ) alone or in combination with azithromycin (AZ) is one of the many therapies being explored for the treatment of Coronavirus 2019 (COVID-19). We performed a systematic review regarding the effects of HCQ versus HCQ+AZ on corrected QT interval (QTc) and cardiovascular outcomes. Methods: We performed a systematic search, using PubMed, EMBASE, SCOPUS, and Google Scholar from inception to May 3rd, 2020, with studies fulfilling the following inclusion criteria: (1) compared HCQ versus HCQ+AZ in COVID-19; (2) reported change in QTc interval and/or cardiovascular outcomes. The primary outcome was change in QTc (maximum QTc–baseline QTc) and incidence of TdP in COVID-19 patients on HCQ vs. HCQ+AZ. Results: A statistically significant change in QTc interval was observed with HCQ+AZ compared to HCQ alone (WMD 9.13 ms, 95%CI 3.74-14.01, p=0.01, I2=29.04%). However, no significant difference in the risk of development of QTc>500 ms was observed between two groups (10.6% in HCQ vs. 14.7% in HCQ+AZ, RR 0.71, 95% CI 0.32-1.59, p =0.40, I2 = 35.8%). Also, no significant difference in risk of TdP was observed between the two groups (0% vs. 0.5%, risk difference -0.002,95% CI-0.02 to 0.02, p=0.83, I2 =0%, respectively). However, one patient experienced TdP, three days after discontinuation of HCQ+AZ for prolonged QTc (499 ms). Conclusion: The risk/benefit of HCQ and AZ should be carefully contemplated, given the risk of QTc prolongation. Until further safety data is available, we recommend close monitoring of QTc interval and electrolytes, avoiding drug-drug interactions in these high-risk patient populations.