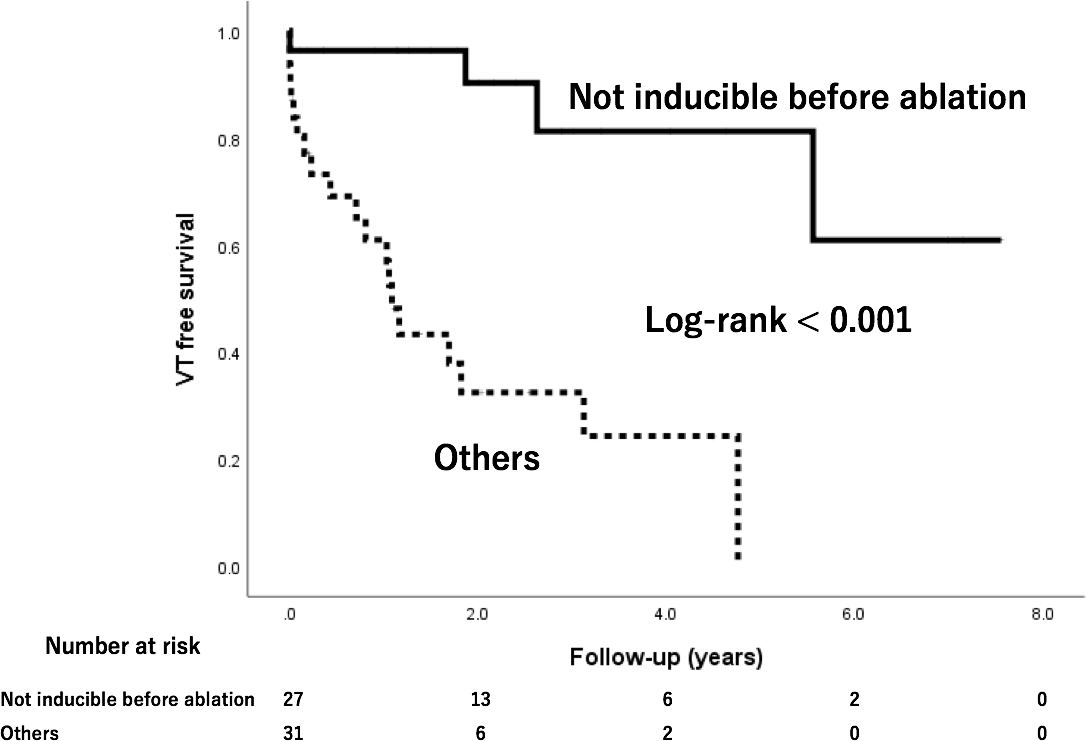
Background: Ventricular arrhythmia inducibility is one of the ideal endpoints of ventricular tachycardia(VT) ablation. However, it may be challenging to implement programmed electrical stimulation (PES) at the end of the procedure under several circumstances. The long-term outcome of patients who did not undergo PES after VT ablation remains largely unknown. Purpose: To investigate the details and long-term outcome of VT ablation in patients who did not undergo PES at the end of the ablation procedure. Methods: Among 184 VT ablation procedures in patients with structural heart disease who underwent VT ablation using an irrigated catheter, we enrolled those who did not undergo PES after VT ablation. VT ablation strategy involved targeting induced VT plus pacemap-guided substrate ablation if inducible. If VT was not inducible, substrate-based ablation was performed. The primary endpoint was VT recurrence. Results: In 58 procedures, post-ablation VT inducibility was not assessed. The causes were non-inducibility of sustained VT before ablation(27/58, 46.6%), long procedure time(27.6%, mean 392 min), complications(10.3%), intolerant hemodynamic state(10.3%), and inaccessible or unsafe target(6.9%). With regard to the primary endpoint, 23 recurrences(39.7%) were observed during a mean follow-up period of 2.5 years. Patients with non-inducibility before ablation showed less VT recurrences(4/27, 14.8%) during follow-up than patients with other causes of untested PES after ablation(19/31, 61.2%)(Log-rank<0.001). Conclusions: VT recurrence was not observed in approximately 60% of the patients who did not undergo PES at the end of the ablation procedure. PES after VT ablation may be not needed among patients with pre-ablation non-inducibility.