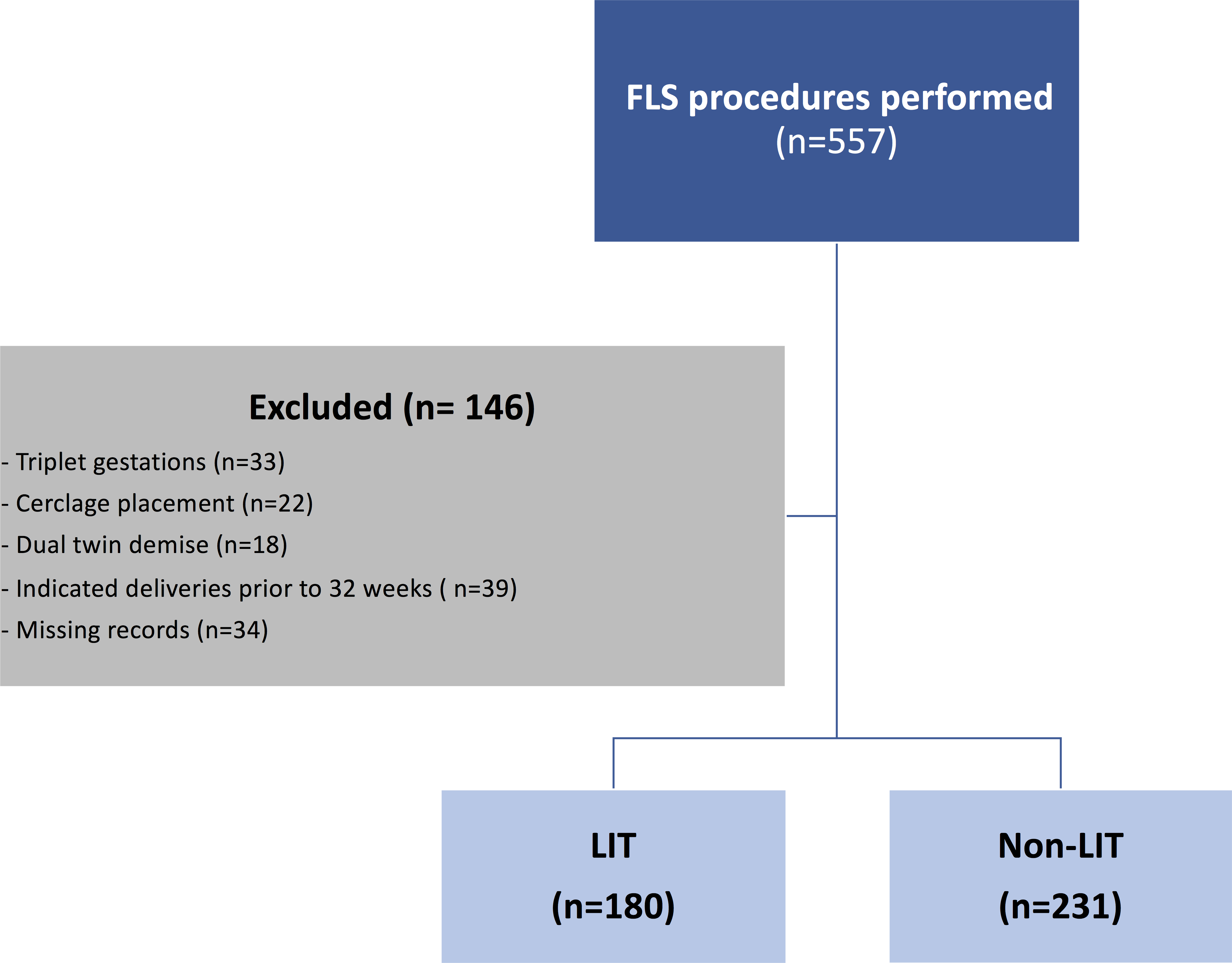
Objective: To evaluate the efficacy of long-term indomethacin therapy (LIT) in prolonging pregnancy and reducing spontaneous preterm birth (PTB) in patients undergoing fetoscopic laser surgery (FLS) for the management of twin-to-twin transfusion syndrome (TTTS). Design: Retrospective cohort study of prospectively collected data. Setting: Collaborative multicenter study Population: 557 consecutive TTTS cases that underwent FLS Methods: LIT was defined as indomethacin use for at least 48 hours. Log-binomial regression was used to estimate the relative risk (RR) of PTB in LIT compared to non-LIT group. Cox regression was used to evaluate the association between LIT use and FLS-to-delivery survival. Main outcome measures: gestational age (GA) at delivery Results: Among the 411 pregnancies included, a total of 180 patients (43.8%) received LIT after FLS and 231 patients (56.2%) did not. Median GA at fetal intervention did not differ between groups (20.4 weeks). Median GA at delivery was significantly higher in the LIT group (33.6 weeks) compared to the non-LIT group (31.1weeks), p<0.001. FLS-to-delivery interval was significantly longer in the LIT group (P<0.001). The risk of PTB prior to 34, 32, 28, and 26 weeks gestation were all significantly lower in the LIT group compared to the non-LIT group (RR=0.69, 0.51, 0.37, and 0.18, respectively). The number needed to treat (NNT) with LIT to prevent one PTB<32 weeks gestation was 4, and to prevent one PTB<34 weeks was 5. Conclusion: Long-term indomethacin after FLS for TTTS was found to be associated with prolongation of pregnancy and reducing the risk for PTB.