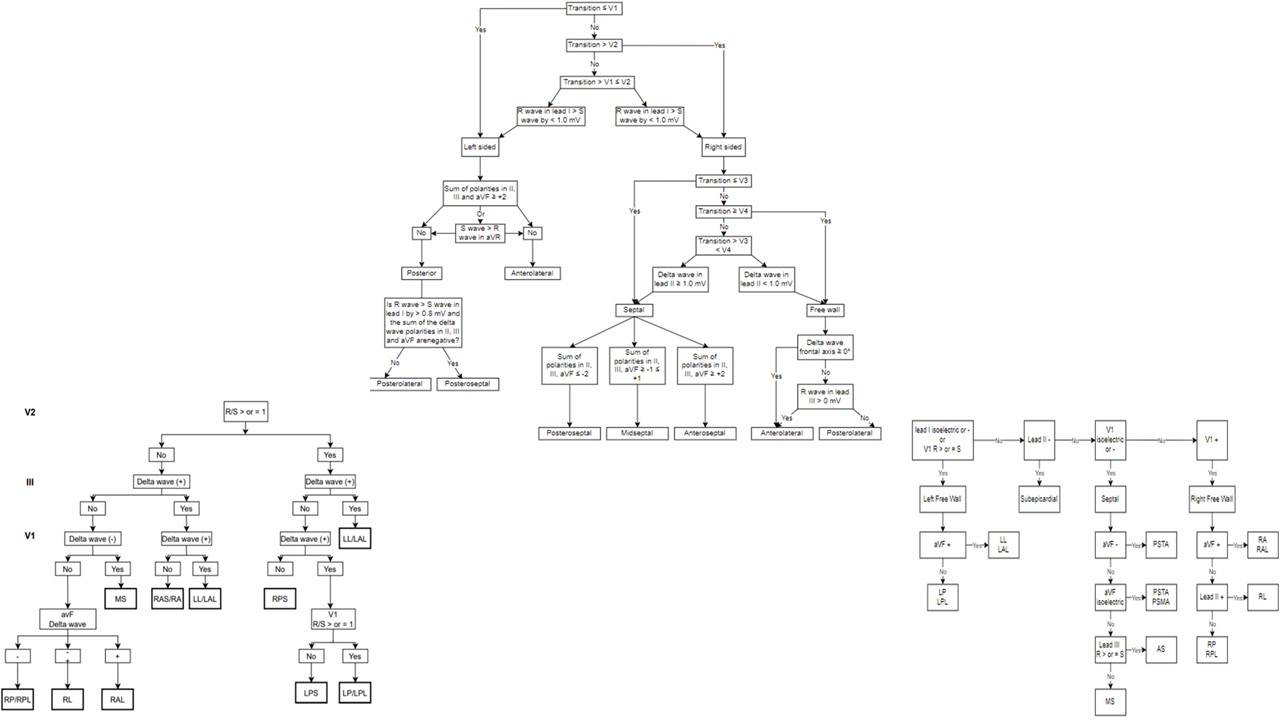
Is there a need for a novel algorithm for accessory pathways localization?Malek Nayfeh MD, Marwan M. Refaat MDDivision of Cardiology, Department of Internal Medicine, American University of Beirut Medical Center, Beirut, LebanonRunning Title: Is there a need for a novel algorithm for WPW localization?Words: 572 (excluding the title page and references)Keywords: accessory pathways, Wolff-Parkinson-white, WPW, cardiac arrhythmias, cardiovascular diseases, heart diseases, Inferior Lead DiscordanceFunding: NoneDisclosures: NoneCorresponding Author:Marwan M. Refaat, MD, FACC, FAHA, FHRS, FASE, FESC, FACP, FRCPAssociate Professor of MedicineDirector, Cardiovascular Fellowship ProgramDepartment of Internal Medicine, Cardiovascular Medicine/Cardiac ElectrophysiologyDepartment of Biochemistry and Molecular GeneticsAmerican University of Beirut Faculty of Medicine and Medical CenterPO Box 11-0236, Riad El-Solh 1107 2020- Beirut, LebanonUS Address: 3 Dag Hammarskjold Plaza, 8th Floor, New York, NY 10017, USAOffice: +961-1-350000/+961-1-374374 Extension 5353 or Extension 5366 (Direct)Wolff Parkinson White Syndrome (WPW) affects between 0.1% and 0.2% of the population, causes morbidity due to supraventricular tachycardia (SVT) and can lead to sudden cardiac arrest [1-3]. The management involves localizing the accessory pathway, and then ablating it, by using either radiofrequency (RF) ablation or cryoablation. The electrocardiogram has been useful over the last decades in the localization of accessory pathways, premature ventricular contractions site of origin and pacing sites [4]. Regarding localization of the pathway, following a large study of RF ablation, Fitzpatrick et al described eight anatomical locations of different pathways using fluoroscopic landmarks: Right anteroseptal (RAS), right midseptal (RMS), right posteroseptal (RPS), right anterolateral (RAL), right posterolateral (RPL), left anterolateral (LAL), left posterolateral (LPL) and left posteroseptal (LPS) [5]. Other algorithms such as the Arruda algorithm or the D’Avila algorithm are also used by clinicians [6, 7]. Most of the accessory pathways’ localization algorithms involve assessment of the delta wave vector (Figure 1), some focus more on QRS morphology (Figure 2), and others combine both methods (Figure 3) [8-12]. By using these algorithms, differentiating between right sided and left sided accessory pathways does not generally pose a problem. However, determining the exact location of right and left sided pathways appears to be more challenging.The study of Bera et al. is a retrospective cohort. Twenty-two patients met the inclusion criteria. The aim was to assess the value of inferior lead discordance (meaning a positive QRS in lead II and a negative QRS in lead III) as a predictor of right anterior (RA) and RAL pathway. The authors included participants who had undergone RF ablation and were found to have right sided pathways. They then separated them in two groups based on if they had RA and RAL pathway (group 1) vs other pathways (group 2). The study found that all patients who had RA and RAL pathway had an ECG showing ILD, while 17 out of 18 patients who were in the other locations did not have an ECG with ILD. The sensitivity and specificity of ILD for predicting RAL location are 100% and 95% respectively.The findings in this study are highly relevant because they represent a clear and simple way of localizing RA/RAL pathways. Other algorithms are also extremely helpful but have their limitations especially if they rely on the delta wave polarity and the electrocardiogram is not fully pre-excited. Another advantage to the algorithm used in this study is that it focuses on limb leads, instead of pericardial leads, which are highly susceptible to variability due to possible displacement.This was a well conducted study, but has some limitations, most notably the small sample size of 22, with only 4 being RA and RAL pathways. There are many algorithms that help cardiologists and cardiac electrophysiologists in localizing accessory pathways before ablation, however, none has specifically focused on RA and RAL pathways. With the advances in artificial intelligence and machine learning, more algorithms using them might be developed in the future.Figure LegendsFigure 1: Examples of algorithms that rely on delta wave polarity such as Fitzpatrick (top) [5], Chiang (bottom left) [8] and Arruda (bottom right) [6]Figure 2: Example of algorithms that rely on QRS morphology such as D’Avilla (top left) [7], Taguchi (top right) [9] and St George’s (bottom) [10].Figure 3: Examples of algorithms that rely both on delta waves and QRS morphology, such as Pambrun (top) [11] and Baek (bottom) [12].References:1. Refaat MM, Hotait M, Tseng ZH (2014). Utility of the Exercise Electrocardiogram Testing in Sudden Cardiac Death Risk Stratification. Ann Noninvasive Electrocardiol, 19(4): 311-318.2. Lu, C. W., Wu, M. H., Chen, H. C., Kao, F. Y., & Huang, S. K. (2014). Epidemiological profile of Wolff-Parkinson-White syndrome in a general population younger than 50 years of age in an era of radiofrequency catheter ablation. International journal of cardiology, 174(3), 530–534. https://doi.org/10.1016/j.ijcard.2014.04.1343. Arai, A., & Kron, J. (1990). Current management of the Wolff-Parkinson-White syndrome. The Western journal of medicine, 152(4), 383–391.4. Refaat M, Mansour M, Singh JP, Ruskin JN, Heist EK (2011). Electrocardiographic Characteristics in Right Ventricular Versus Biventricular Pacing in Patients With Paced Right Bundle Branch Block QRS Pattern. J Electrocardiol, 44 (2): 289-95.5. Fitzpatrick, A. P., Gonzales, R. P., Lesh, M. D., Modin, G. W., Lee, R. J., & Scheinman, M. M. (1994). New algorithm for the localization of accessory atrioventricular connections using a baseline electrocardiogram. Journal of the American College of Cardiology, 23(1), 107–116. https://doi.org/10.1016/0735-1097(94)90508-86. Arruda, M. S., McClelland, J. H., Wang, X., Beckman, K. J., Widman, L. E., Gonzalez, M. D., Nakagawa, H., Lazzara, R., & Jackman, W. M. (1998). Development and validation of an ECG algorithm for identifying accessory pathway ablation site in Wolff-Parkinson-White syndrome. Journal of cardiovascular electrophysiology, 9(1), 2–12. https://doi.org/10.1111/j.1540-8167.1998.tb00861.x7. d’Avila, A., Brugada, J., Skeberis, V., Andries, E., Sosa, E., & Brugada, P. (1995). A fast and reliable algorithm to localize accessory pathways based on the polarity of the QRS complex on the surface ECG during sinus rhythm. Pacing and clinical electrophysiology : PACE, 18(9 Pt 1), 1615–1627. https://doi.org/10.1111/j.1540-8159.1995.tb06983.x8. Chiang, C. E., Chen, S. A., Teo, W. S., Tsai, D. S., Wu, T. J., Cheng, C. C., Chiou, C. W., Tai, C. T., Lee, S. H., & Chen, C. Y. (1995). An accurate stepwise electrocardiographic algorithm for localization of accessory pathways in patients with Wolff-Parkinson-White syndrome from a comprehensive analysis of delta waves and R/S ratio during sinus rhythm. The American journal of cardiology, 76(1), 40–46. https://doi.org/10.1016/s0002-9149(99)80798-x9. Taguchi, N., Yoshida, N., Inden, Y., Yamamoto, T., Miyata, S., Fujita, M., Yokoi, K., Kyo, S., Shimano, M., Hirai, M., & Murohara, T. (2013, December 22). A simple algorithm for localizing accessory pathways in patients with Wolff-Parkinson-White syndrome using only the R/S ratio. Journal of Arrhythmia. Retrieved February 10, 2022, from https://www.sciencedirect.com/science/article/pii/S188042761300165810. Xie, B., Heald, S. C., Bashir, Y., Katritsis, D., Murgatroyd, F. D., Camm, A. J., Rowland, E., & Ward, D. E. (1994). Localization of accessory pathways from the 12-lead electrocardiogram using a new algorithm. The American journal of cardiology, 74(2), 161–165. https://doi.org/10.1016/0002-9149(94)90090-611. Pambrun, T., El Bouazzaoui, R., Combes, N., Combes, S., Sousa, P., Le Bloa, M., Massoullié, G., Cheniti, G., Martin, R., Pillois, X., Duchateau, J., Sacher, F., Hocini, M., Jaïs, P., Derval, N., Bortone, A., Boveda, S., Denis, A., Haïssaguerre, M., & Albenque, J. P. (2018). Maximal Pre-Excitation Based Algorithm for Localization of Manifest Accessory Pathways in Adults. JACC. Clinical electrophysiology, 4(8), 1052–1061. https://doi.org/10.1016/j.jacep.2018.03.01812. Baek, S. M., Song, M. K., Uhm, J. S., Kim, G. B., & Bae, E. J. (2020). New algorithm for accessory pathway localization focused on screening septal pathways in pediatric patients with Wolff-Parkinson-White syndrome. Heart rhythm, 17(12), 2172–2179. https://doi.org/10.1016/j.hrthm.2020.07.016.