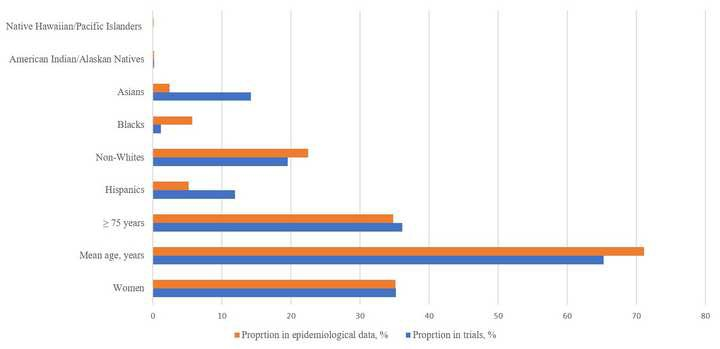
Background: Representation trends of women, older adults, and ethnic/racial minorities in randomized controlled trials (RCTs) of atrial fibrillation (AF) are uncertain. Methods: We systematically reviewed 134 AF related RCTs (phase II and III) encompassing 149,162 participants using Medline and ClinicalTrials.gov through April 2019 to determine representation trends of women, older patients (≥ 75 years), and ethnic/racial minorities. Weighted data on the prevalence of AF from epidemiological studies were used to compare the representation of the studied groups of interest in AF RCTs to their expected burden of the disease. Results: Only 18.7% of the RCTs reported proportion of older patients, and 12.7% RCTs reported ethnic/racial minorities. In RCTs, proportions of women, Hispanics, Blacks, American Indian/Alaskan patients, Asians, native Hawaiian/Pacific Islanders and non-Whites were 35.2%, 11.9%, 1.2%, 0.2%, 14.2%, 0.05%, and 19.5%, respectively. The corresponding proportions in general population were 35.1%, 5.2%, 5.7%, 0.2%, 2.4%, 0.1%, and 22.5%, respectively. The weighted mean age (SD) across the trials was 65.3 (3.2) years which was less than the corresponding weighted mean age of 71.1 (4.5) years in the comparative epidemiological data. Conclusion: The reporting of older patients and ethnic/racial minorities was poor in RCTs of AF. The representation of women and American Indian/Alaskan natives matched their expected population share of disease burden. Hispanics and Asians were over-represented and Blacks, native Hawaiian/Pacific Islanders and non-Whites were under-represented in RCTs of AF. In nearly all studied RCTs, the reporting of racial demographics did not start until later part of last decade.