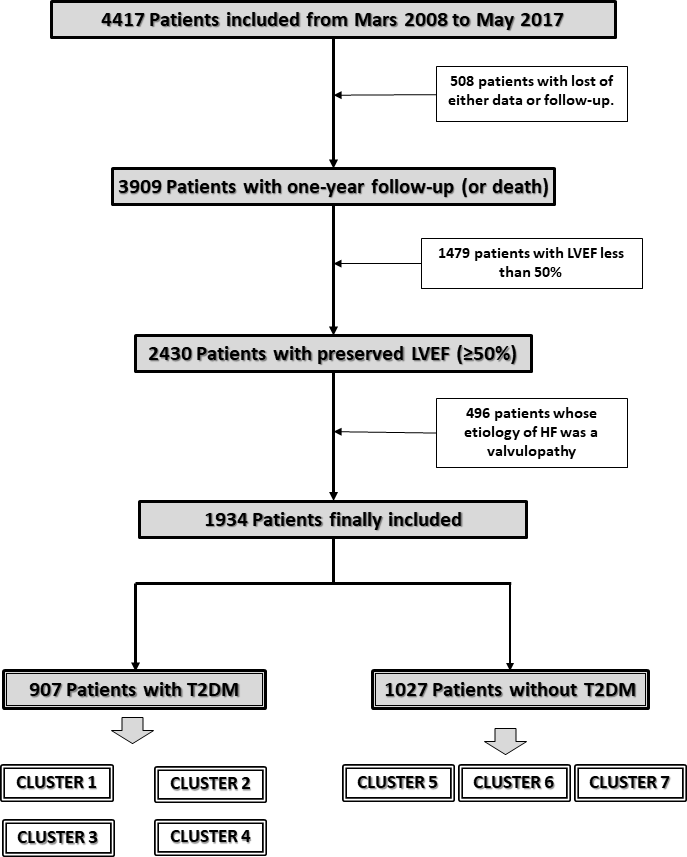
AIM: to determine if patients with heart failure and preserved ejection fraction (HFpEF) and type 2 diabetes mellitus (T2DM) have a higher comorbidity burden than those without T2DM, if other comorbidities are preferentially associated with T2DM, and if these conditions confer a worse patient prognosis. METHODS AND RESULTS: Cohort study based on the RICA Spanish Heart Failure Registry, a multicenter, prospective registry that enrolls patients admitted for decompensated HF and follows them for 1 year. We selected only patients with HFpEF, classified as having or not having T2DM, and performed an agglomerative hierarchical clustering based on variables such as the presence of arrhythmia, chronic obstructive pulmonary disease, dyslipidemia, liver disease, stroke, dementia, body mass index (BMI), hemoglobin levels, estimated glomerular filtration rate, and systolic blood pressure. 1,934 patients were analyzed: 907 had T2DM (mean age 78.4+/-7.6 years) and 1,027 did not (mean age 81.4+/- 7.6 years). The analysis resulted in 4 clusters in patients with T2DM, and 3 in the reminder. All clusters of patients with T2DM showed higher BMI, and more kidney disease and anemia than those without T2DM. Clusters of patients without T2DM had neither significantly better nor worse outcomes. However, among the T2DM patients, clusters 2, 3 and 4 all had significantly poorer outcomes, the worst being cluster 3 (HR 2.0, 95% CI 1.36-2.93, p=0.001). CONCLUSIONS: Grouping our patients with HFpEF and T2DM into clusters based on comorbidities revealed a greater disease burden and prognostic implications associated with the T2DM phenotype, compared to those without T2DM.