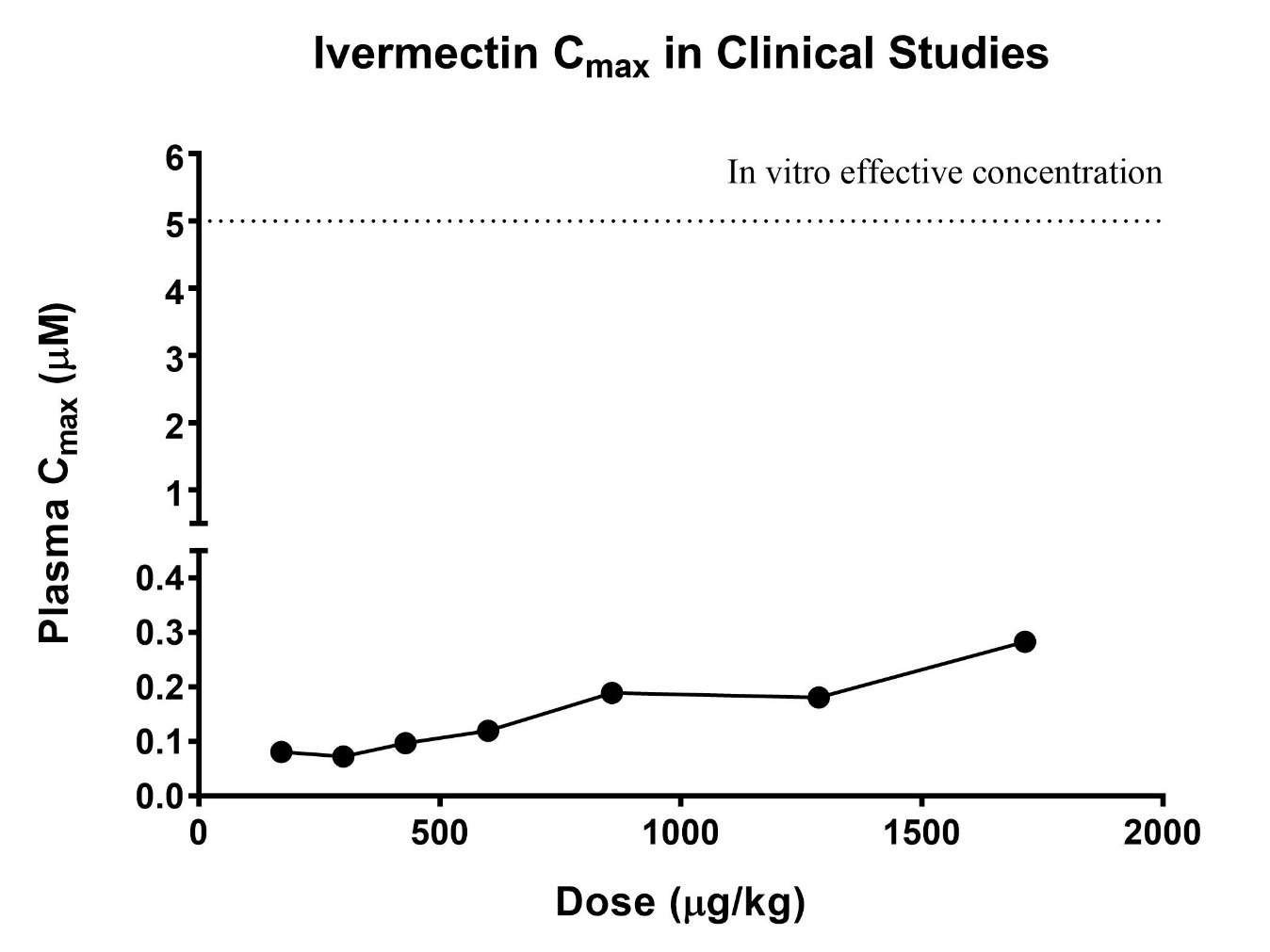
Hundreds of researchers are working to develop a vaccine and are evaluating drugs to mitigate the adverse health and economic consequences of COVID-19 (Coronavirus disease 19) worldwide. If novel compounds are found, geopolitical and economic variables will determine their introduction to communities. Therefore, finding low-cost and widely accessible drugs for prevention or treatment of COVID-19 would be ideal.A recent study found that ivermectin, an FDA-approved anti-parasitic drug, has inhibitory effects on replication of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)1. Ivermectin has broad anti-viral activity through inhibition of viral proteins including importin α/β1 heterodimer and integrase protein2. Caly and colleagues reported that the addition of ivermectin at a concentration of 5 micromolar (μM) (twice the reported IC50) to Vero-hSLAM cells, 2 hours post infection with SARS-CoV-2, resulted in a reduction in the viral RNA load by 99.98% at 48 hours1. The authors suggested that this drug could reduce the viral load in infected patients, with potential effect on disease progression and spread.While the findings by Caly and colleagues provide some promise, there is no evidence that the 5 μM concentration of ivermectin used by Caly and colleagues in their in vitro SARS-CoV-2 experiment, can be achieved in vivo . The pharmacokinetics of ivermectin in humans is well described (Figure 1)3-5, and even with the highest reported dose of approximately 1700 µg/kg (i.e. 8.5 times the FDA-approved dose of 200 μg/kg), the maximum plasma concentration was only 0.28 µM5. This is 18 times lower than the concentration required to reduce viral replication of SARS-CoV-2in vitro . Ivermectin accumulation in tissues is mild and would not be sufficient to achieve the antiviral effect with conventional doses6. Although high doses of ivermectin in adults or children are well tolerated5,7, the clinical effects of ivermectin at a concentration of 5 μM range are unknown and may be associated with toxicity. Consequently, ivermectin has in vitroactivity against SARS-CoV-2 but this effect is unlikely to be observedin vivo using current dosing.Amidst fear of the pandemic, the public and some physicians are now using ivermectin off-label for prophylaxis or as adjuvant therapy for COVID-19. Because ivermectin is only commercially available as a 3 or 6 mg tablets or a 6 mg/ml oral suspension, in order to administer a high dose, some people may experiment with more concentrated veterinary formulations. These actions are not based on clinical trials and have motivated cautionary statements from institutions such as the FDA against the use of pharmaceutical formulations of ivermectin intended for animals as therapeutics in humans 8.Potential avenues for further investigation into repurposing ivermectin for SARS-CoV-2 may be to: (i) develop an inhaled formulation to efficiently deliver a high local concentration in the lung, whilst minimizing systemic exposure; and (ii) evaluate more potent ivermectin analogs (e.g. doramectin) which may also inhibit SARS-CoV-2. These are areas for research – clearly, further studies are needed before ivermectin can be used for the prevention and treatment of COVID-19. As recently discussed in BJCP, this highlights the critical need to consider pharmacological principles to guide in vitro testing when repurposing old drugs for therapeutic use against COVID-199.