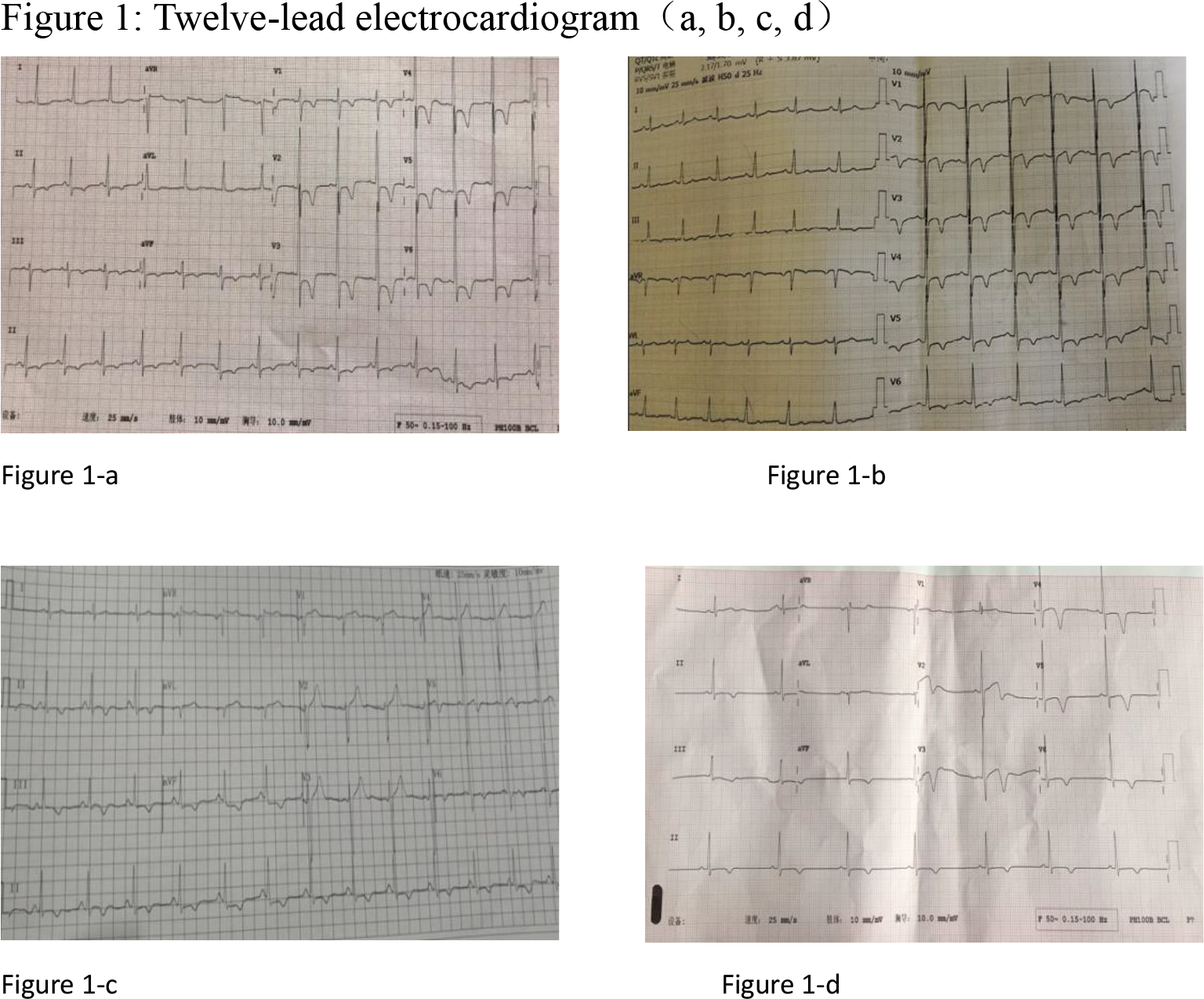
To summarize and analyze the clinical features of Apical hypertrophic cardiomyopathy (ApHCM) which was misdiagnosed before the gross deformity of the papillary muscles and moved down to the apex of the heart due to the presence of Giant Negative T-wave (GNT). The clinical data of 215 patients who were previously diagnosed with ApHCM due to the presence of GNT in our hospital from 2006 to 2018 were retrospectively analyzed. Results: After careful observation and combined with LVO examination, 11 cases were found to have clinical features of large papillary muscle deformity and the position was moved down to the apex (ADPM). 9 cases of them were: anterior wall myocardial ischemia, patients with 6–14mm T wave inversion in leads V4-V6; 2 cases of inferior wall ischemia, middle-aged male patients with recurrent chest tightness, shortness of breath1 More than hours, especially after fatigue. ECG tips: sinus rhythm, normal ECG axis, 6-10mm T wave inversion, no abnormal angiography, echocardiography shows left ventricular wall structure, exercise, and left ventricular ejection fraction (LVEF) Within normal range. Echocardiography showed that the papillary muscles were thick and moved down, and the GNT corresponded to leads II, III, and AVF. This report shows that the huge negative T wave is not a specific manifestation of myocardial ischemia. The diagnosis is ApHCM is a misdiagnosis. Abnormal papillary muscle location and papillary muscle morphology can also lead to the occurrence of GNT.