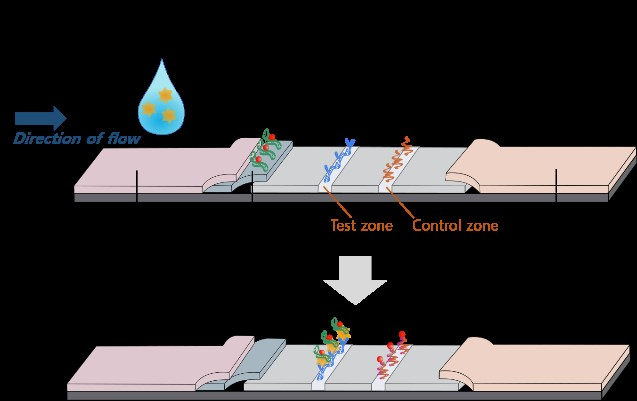
Objective: Nephrin is a protein in the glomerular podocyte slit diaphragm; therefore, its presence in urine implies damage to podocytes. This study aimed to determine the efficacy of nephrin as a biomarker in maternal urine to predict preeclampsia (PE). Design and setting: This prospective study included pregnant women admitted for delivery at Seoul National University Bundang Hospital: March 2019 – May 2020. Population: Patients who had been diagnosed with PE were included and patients without a history of underlying diseases were recruited for the control group. Important clinical data has been collected. Methods: Urine samples were obtained, and nephrin signaling was detected through test strips using a lateral flow assay. Main Outcome Measures: The results of the point-of-care test were compared between the 2 groups: patients with PE, and without (control group) using the exact concentration of nephrin by enzyme-linked immunosorbent assay (ELISA). Results: Clinical characteristics – maternal age, rate of nulliparity, proportion of twin pregnancies, height, weight, cesarean section rate – were comparable between the PE and control groups. Nephrin signals were classified into four groups. In the PE group, signals 0, 1, 2, and 3 were found in 18.4% (9/49), 44.9% (22/49), 24.5% (12/49), and 12.2% (6/49) of participants, respectively. This was significantly different from the control group, in which 84.3% (43/51) were found to have signal 0 (P<0.001). Conclusions: Nephrin signaling in maternal urine could be a noninvasive and useful test for predetecting severity of PE.