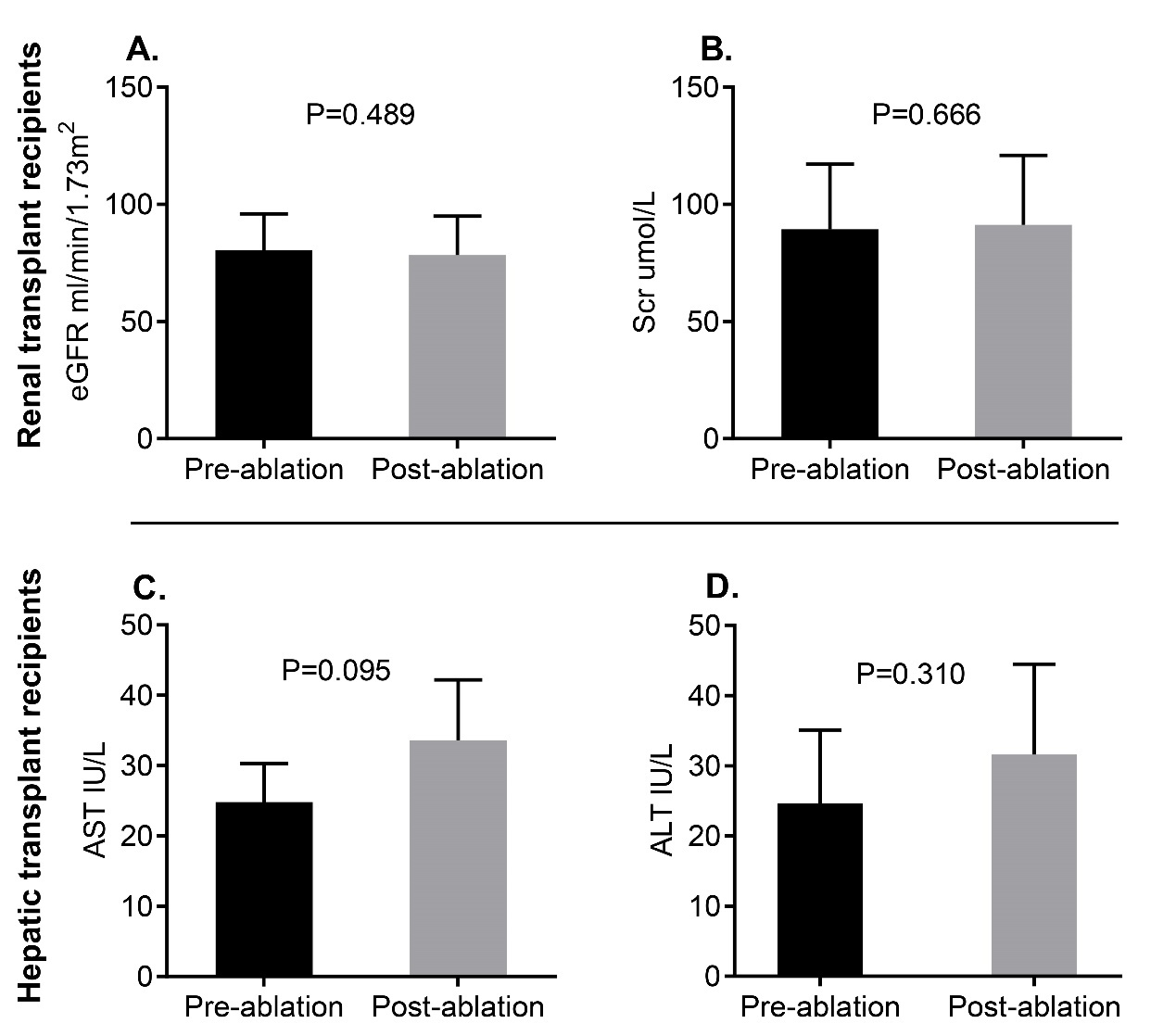
Background: Atrial fibrillation (AF) is common in abdominal solid organ transplant recipients and a cause of morbidity and mortality in this population. However, the outcomes of catheter ablation (CA) in transplant recipients with AF remain unclear. This study aimed to elucidate the outcomes of CA in renal and hepatic transplant recipients. Methods and Results: Between 2015 and 2019, 14 transplant recipients (9 with kidney transplantation and 5 with liver transplantation) were enrolled from among 10,741 AF patients and underwent CA at Anzhen Hospital. Another 56 patients matched by age, sex and AF type were selected as the control group (4 controls for each transplant recipient). During a mean follow-up of 30.0±13.3 months after the initial procedure, 10 (71.4%) of the transplant patients, compared to 41 (73.2%) of the control patients, remained free from AF recurrence(P=1.000). A repeated procedure was performed in 1 transplant patient and in 6 control subjects. Consequently, 11 (78.6%) of the transplant patients, compared to 46 (82.1%) of controls, were in sinus rhythm after the repeated ablation (P=0.715). Notably, Kaplan–Meier analysis did not demonstrate any significant differences in the atrial arrhythmia-free rate after the initial and repeated procedure between the two groups. Vascular complications were identified in 1 transplant patient and 2 control subjects, while no life-threatening complications were observed in either group. There was no transient allograft dysfunction in transplant recipients after CA. Conclusion: CA is safe and effective in abdominal solid transplant recipients, and may be an optimal therapeutic strategy for this group.