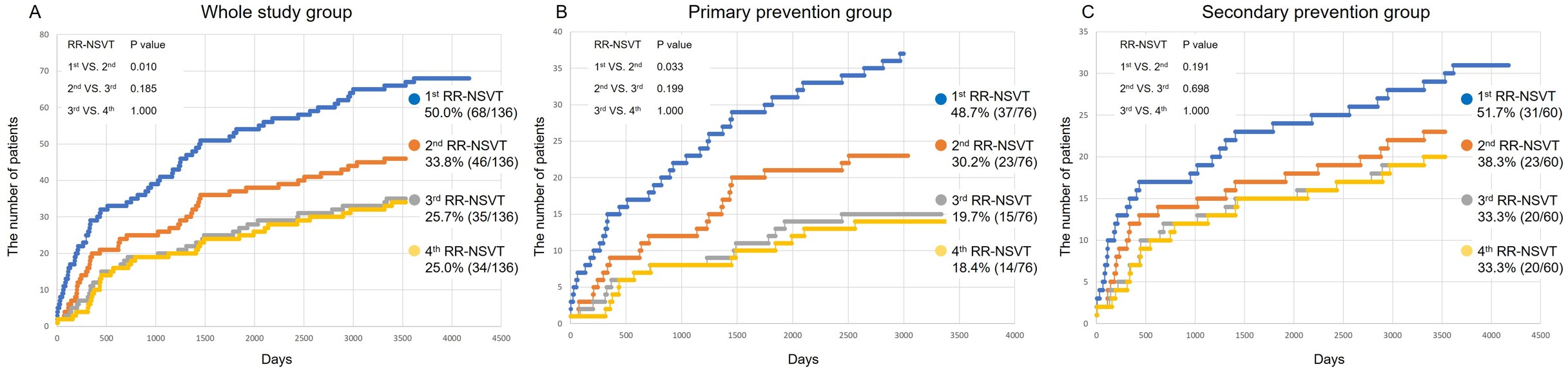
Aims Non-sustained ventricular tachycardia (NSVT) occurs frequently in patients with dilated cardiomyopathy (DCM), especially in high-risk patients. The role of rapid-rate NSVT (RR-NSVT) documented by an implantable cardioverter defibrillator (ICD) in DCM patients has not been fully explored. This study aimed to determine the relationship between RR-NSVT and the occurrence of ventricular tachyarrhythmias (VTAs) in DCM patients with ICD. Methods From December 2000 to December 2017, 136 DCM patients received ICD or cardiac resynchronization therapy defibrillator (CRT-D) implantation for primary or secondary prevention of VTAs. Based on the occurrence of documented RR-NSVT, patients were classified into RR-NSVT (-) or RR-NSVT (+) groups. Result During the median follow-up of 4.5 years, 50.0% (68/136) of patients experienced ≥ 1 episode, and 25.0% (34/136) of patients experienced ≥ 3 episodes of RR-NSVT. Event-free survival for VTAs was significantly higher in the RR-NSVT (+) group whereas those for heart failure admission and cardiovascular mortality were comparable between groups. In the multivariate cox regression analysis, any RR-NSVT showed a positive association with the occurrence of VTAs (HR: 5.087; 95% CI: 2.374-10.900; p<0.001). In RR-NSVT (+) patients, a cluster (≥ 3 times/6 months) and frequent pattern (≥ 3 runs/day) of RR-NSVT were observed in 42.6% (29/68) and 30.9% (21/68) of patients, respectively, who showed further increased incidence of VTAs. Conclusion In DCM patients with ICD/CRT-D, 50.0% experienced at least 1 episode of RR-NSVT. RR-NSVT documentation showed a positive association with subsequent occurrence of VTAs, suggesting the importance of constructive arrhythmia management for patients with RR-NSVT.