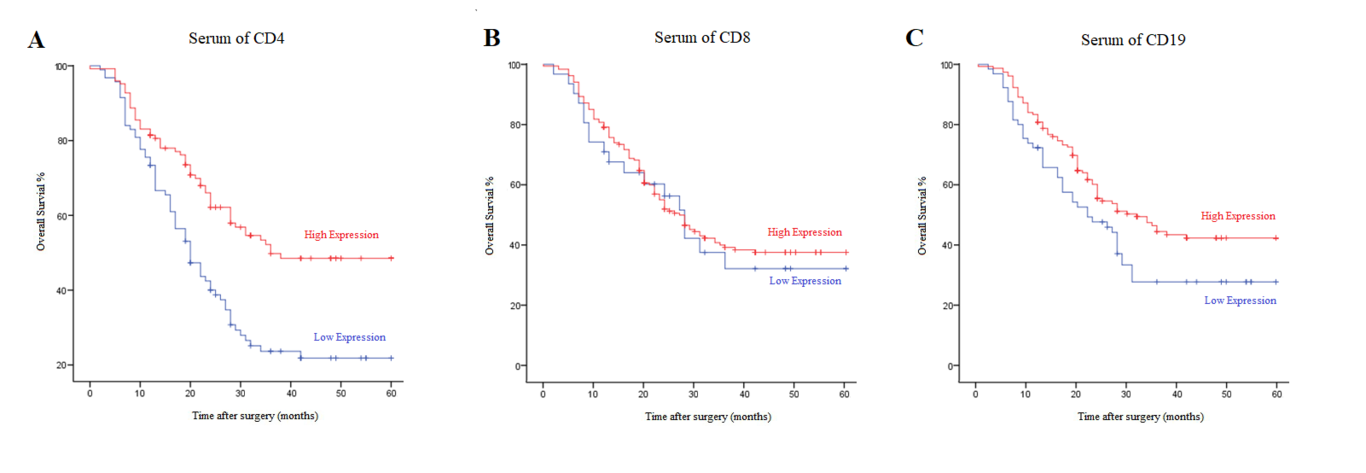
Serum CD4, CD8 and CD19 are markers of systemic inflammation. However, there is little evidence on the influence of inflammation on the tumor microenvironment and the prognostic indicators of gastric cancer (GC). In this study, two hundred and eight patients who underwent radical gastrectomy for GC were included. Preoperative peripheral blood samples were used to analyze serum CD4, CD8 and CD19. The optimal cutoff levels for CD4, CD8 and CD19 were defined by receiver operating characteristic curve analysis (CD4=38.85%, CD8=14.35% and CD19=7.40%). The areas with specific CD4+T cells, CD8+T cells and CD19+B cells within the tumor microenvironment were measured in paraffin sections by immunohistochemistry and analyzed by Image-Pro Plus. 94 patients had low CD4 and 124 patients had high CD4 levels. 31 patients had low CD8 and 187 patients had high CD8 levels. 64 patients had low CD19 and 154 patients had high CD19 levels. Infiltration of CD4+T cells was associated with serum CD4 (P<0.001). Serum CD4, CD19, and the infiltration of CD4+T cells, CD8+T cells, and CD19+B cells were significant in predicting the prognosis of GC. Low CD4 level, infiltration of CD8+T cells and high infiltration of CD4+T cells and CD19+B cells were correlated with worse overall survival in multivariate analysis. Collectively, our results provide evidence that serum CD4 is associated with the infiltration of CD4+T cells in the tumor microenvironment, which indicates the prognostic value of systemic inflammation in GC.